दुनिया के बेहद ठंडे इलाकों में रहने वाले प्यारे से जीव अब शरणार्थी बन गए हैं. इन जीवों को अब दूसरी जगहों पर आशियाना खोजना पड़ रहा है. हाल ही में रूस के वैज्ञानिकों ने वॉलरस (Walrus) नामक जीवों की एक बड़ी कॉलोनी को खोजा जो अपने वास्तविक रिहायशी इलाके से दूर थे. इस कॉलोनी में करीब 3000 वॉलरस मौजूद थे. आइए जानते हैं कि आखिरकार इन्हें अपना घर क्यों छोड़ना पड़ा और ये विस्थापितों का जीवन जीने के लिए क्यों मजबूर हो रहे हैं।
रूसी वैज्ञानिकों ने देखा कि 3000 वॉलरस एक साथ रूस के यमल प्रायद्वीप के सुदूर और शांत इलाके में एक साथ मौजूद हैं. ये यहां पर अपना सामाजिक ताना-बाना बनाते दिख रहे हैं. प्रजनन क्रिया में व्यस्त हैं. लेकिन आमतौर पर इन कार्यों के लिए ये कारा सागर मैं तैरते हुए बर्फ के टुकड़ों पर जाते हैं. जबकि, इस बार ये प्यारे से जीव करीब 600 किलोमीटर दूर तट पर आ गए हैं।
आर्कटिक सर्किल पर शोध कर रहे रूसी वैज्ञानिक एलेक्जेंडर सोकोलोव ने बताया कि यह अद्भुत नजारा है. आमतौर पर प्रजनन या सामाजिक गठजोड़ के लिए ये जीव कारा सागर में मौजूद बर्फ के टुकड़ों पर जाते थे. इस बार, ये तट पर आ गए हैं. यानी कारा सागर में इतना बड़ा समुद्री बर्फ का टुकड़ा नहीं बचा जहां ये अपनी निजी और सामाजिक जीवन को जी सकें।
इस कॉलोनी में नर, मादा के साथ-साथ हर उम्र के शावक भी हैं. एलेक्जेंडर ने बताया कि इन जीवों का अध्ययन करने के लिए यह एक खुली प्रयोगशाला जैसा है. इंटरनेशनल यूनियन फॉर कंजरवेशन ऑफ नेचर ने साल 2016 में वॉलरस जीवों को लगभग लुप्तप्राय की सूची में डाला था. दुनिया भर में इनकी आबादी करीब 12,500 के आसपास है।
इनके शिकार पर अंतरराष्ट्रीय स्तर पर प्रतिबंध लगा हुआ है लेकिन चोरी-छिपे इनका शिकार किया जाता है. इनके दांत और चमड़े का अवैध कारोबार किया जाता है. मैरीन मैमल रिसर्च एंड एक्सपेडिशन सेंटर के वैज्ञानिक आंद्रेई बोल्टूनोव ने कहा कि अटलांटिक वॉलरस की आबादी तो बढ़ रही है लेकिन इनके रहने की जगह खत्म हो रही है।
आंद्रेई ने कहा कि ग्लोबल वार्मिंग और इंसानी हरकतों की वजह से ये जिस ठंडे इलाके में रहते हैं वहां बर्फ पिघल रही है. इसकी वजह से इन्हें दूसरे इलाकों की तरफ जाना पड़ता है. पिछले कुछ दशकों में कारा सागर में आइस-फ्री सीजन का समय अंतराल बढ़ गया है. इसकी वजह से वॉलरस जीवों को काफी दिक्कतों का सामना करना पड़ता है. (फोटोः गेटी)
वैज्ञानिकों ने कुछ वॉलरस के डीएनए भी लिए हैं. इसके अलावा अलग-अलग कॉलोनियों में मौजूद कुछ वॉलरस की सैटेलाइट टैगिंग की है, ताकि उनके मूवमेंट का पता किया जा सके. इसकी वजह से वॉलरस जीवों के व्यवहार में आने वाले बदलावों का अध्ययन करना आसान हो जाता है।
आंद्रेई ने बताया कि अभी ये पता करना बाकी है कि आखिरकार वॉलरस को यमल प्रायद्वीप का ये तट क्यों पसंद आ रहा है. क्यों ये जीव यहां पर अपनी कॉलोनी बना रहे हैं. ये यहां रहेंगे या फिर वापस बर्फ के टुकड़ों की तलाश में कारा सागर में लंबी यात्रा पर निकल जाएंगे।
आप सभी मेरे साथ जुड़ सकते हैं नीचे दिए गए लिंक पर जाकर और अपने विचार रख सकते हैं। धन्यवाद 🙏
Vitamin A In Winters May Help Burn Fat Faster (Study); Some Foods You Can Eat!!
Weight loss diet: If you believe in these finding and want to replenish your system with vitamin C, here are some foods you can add to your winter diet.
Weight loss diet: Vitamin A-rich foods may be beneficial.Mr. Jatin Tyagi (Certified Nutritionist)
Highlights:-
A study linked sufficient vitamin A level to weight loss in winter.
It was found that cold temperatures and vitamin A can burn fat faster.
Here are some vitamin A-rich foods you can add to your winter diet.
Winters can make many of us lethargic and a bit too lazy to work out. The irony is that we also tend to indulge in fatty and sweet foods, which leads to more weight gain. Only if we could eat to our heart’s content to keep us warm during the chilling weather and still not gain weight, or better still, lose some. This may seem like just a wishful thinking, but what if we tell you that it might actually come true!? Believe it or not, a research found out that sufficient level of vitamin A during winter may promote weight loss. Shocking, right? Well, it is a little hard to believe but you never know this may actually work!
The study published in the journal of Molecular Metabolism claims that cold temperatures coupled with increased Vitamin A could burn the body fat faster. How? Cold temperature and vitamin A are capable of converting white fat, storing excess calories to brown fat, which “stimulates fat burning and heat generation.”
Weight loss can be achieved through a healthy diet.
If you believe in these finding and want to replenish your system with vitamin A, here are some foods you can add to your winter diet
Vitamin A-rich Foods For Winter Diet:
1.Green Leafy Vegetables
Winter produce abounds with greens. Sarson, palak, methi, and so many fresh green vegetable options are available to fill you up with vitamin A.
2. Carrots
Another winter Special Food, carrot available during this season is sweeter and bright red in colour, which makes our meals tastier and prettier.
3. Meat
‘Gorge on your favourite chicken and mutton dishes with liver for great taste and loads of vitamin A.
4. Fish
Another preferred food of non-vegetarians, fish eaten in any form can provide you with a good amount of vitamin A. The season calls for a nice barbeque meal, so grill and enjoy fish along with chicken and mutton, and other meats in your next cookout.
5. Herbs
Stock up your pantry with different herbs like parsley, basil, oregano etc. to add some fresh and striking flavours to your winter meals.
Coming back to the study, one of the study’s lead researchers, Florian Kiefer from the Medical University of Vienna, cautioned against taking large quantities of vitamin A supplements in an effort to lose weight. The best way to go about it is by enriching your diet through these vitamins A-Rich Foods.
Thank you for reading, stay tunned. Keep supporting given below links.
एक महिला को सब्जी मंडी जाना था…उसने जूट का बैग लिया और सड़क के किनारे सब्जी मंडी की और चल पड़ी। तभी पीछे से एक ऑटो वाले ने आवाज़ दी : ‘कहाँ जायेंगी माता जी…?” महिला ने ”नहीं भैय्या” कहा तो ऑटो वाला आगे निकल गया। अगले दिन महिला अपनी बिटिया मानवी को स्कूल बस में बैठाकर घर लौट रही थी…तभी पीछे से एक ऑटो वाले ने आवाज़ दी :— बहनजी चन्द्रनगर जाना है क्या…? महिला ने मना कर दिया।
पास से गुजरते उस ऑटोवाले को देखकर महिला पहचान गई कि ये कल वाला ही ऑटो वाला था। आज महिला को अपनी सहेली के घर जाना था। वह सड़क किनारे खड़ी होकर ऑटो की प्रतीक्षा करने लगी। तभी एक ऑटो आकर रुका :— ”कहाँ जाएंगी मैडम…?” महिला ने देखा ये वो ही ऑटोवाला है जो कई बार इधर से गुज़रते हुए उससे पूंछता रहता है चलने के लिए…महिला बोली :— ”मधुबन कॉलोनी है ना सिविल लाइन्स में, वहीँ जाना है, चलोगे…?”
ऑटोवाला मुस्कुराते हुए बोला :— ”चलेंगें क्यों नहीं मैडम, आ जाइये…! “ऑटो वाले के ये कहते ही महिला ऑटो में बैठ गयी. ऑटो स्टार्ट होते ही महिला ने जिज्ञासावश उस ऑटोवाले से पूछ ही लिया :—”भैय्या एक बात बताइये..? दो-तीन दिन पहले आप मुझे माताजी कहकर चलने के लिए पूछ रहे थे, कल बहन जी और आज मैडम, ऐसा क्यूँ…?” ऑटोवाला थोड़ा झिझककर शरमाते हुए बोला :—”जी सच बताऊँ… आप चाहे जो भी समझेँ पर किसी का भी पहनावा हमारी सोच पर असर डालता है।
आप दो-तीन दिन पहले साड़ी में थीं तो एकाएक मन में आदर के भाव जागे, क्योंकि मेरी माँ हमेशा साड़ी ही पहनती है। इसीलिए मुँह से स्वयं ही “माताजी” निकल गया। कल आप सलवार-कुर्तें में थीँ, जो मेरी बहन भी पहनती है। इसीलिए आपके प्रति स्नेह का भाव मन में जागा और मैंने ”बहनजी” कहकर आपको आवाज़ दे दी। आज आप जीन्स-टॉप में हैं, और इस लिबास में माँ या बहन के भाव तो नहीँ जागते। इसीलिए मैंने आपको “मैडम” कहकर पुकारा।
शिक्षा :- उपर्युक्त कहानी से हमें यह सीख मिलती हैं कि हमारे परिधान (वस्त्र) न केवल हमारे विचारों पर वरन दूसरे के भावों को भी बहुत प्रभावित करते है।
आप सभी मेरे साथ जुड़ सकते हैं नीचे दिए गए लिंक पर जाकर और अपने विचार रख सकते हैं। धन्यवाद 🙏
जब विश्व की सबसे प्राचीन सभ्यता की स्त्रियां अपने सम्पूर्ण वैभव के साथ सज-धज कर अपने आँचल में फल ले कर निकलती हैं तो लगता है जैसे संस्कृति स्वयं समय को चुनौती देती हुई कह रही हो, "देखो! तुम्हारे असँख्य झंझावातों को सहन करने के बाद भी हमारा वैभव कम नहीं हुआ है, हम सनातन हैं, हम भारत हैं। हम तबसे हैं जबसे तुम हो, और जबतक तुम रहोगे तबतक हम भी रहेंगे।" जब घुटने भर जल में खड़ी व्रती की सिपुली में बाल-सूर्य की किरणें उतरती हैं तो लगता है जैसे स्वयं सूर्य बालक बन कर उसकी गोद में खेलने उतरे हैं। स्त्री का सबसे भव्य, सबसे वैभवशाली स्वरूप वही है। इस धरा को "भारत माता" कहने वाले बुजुर्ग के मन में स्त्री का यही स्वरूप रहा होगा।
कभी ध्यान से देखिएगा छठ के दिन जल में खड़े हो कर सूर्य को अर्घ दे रही किसी स्त्री को, आपके मन में मोह नहीं श्रद्धा उपजेगी। छठ वह प्राचीन पर्व है जिसमें राजा और रंक एक घाट पर माथा टेकते हैं, एक देवता को अर्घ देते हैं, और एक बराबर आशीर्वाद पाते हैं। धन और पद का लोभ मनुष्य को मनुष्य से दूर करता है, पर धर्म उन्हें साथ लाता है। अपने धर्म के साथ होने का सबसे बड़ा लाभ यह होता है कि आप अपने समस्त पुरुखों के आशीर्वाद की छाया में होते हैं। छठ के दिन नाक से माथे तक सिंदूर लगा कर घाट पर बैठी स्त्री अपनी हजारों पीढ़ी की अजियासास ननियासास की छाया में होती है, बल्कि वह उन्ही का स्वरूप होती है। उसके दउरे में केवल फल नहीं होते, समूची प्रकृति होती है। वह एक सामान्य स्त्री सी नहीं, अन्नपूर्णा सी दिखाई देती है।
ध्यान से देखिये! आपको उनमें कौशल्या दिखेंगी, उनमें मैत्रेयी दिखेगी, उनमें सीता दिखेगी, उनमें अनुसुइया दिखेगी, सावित्री दिखेगी... उनमें पद्मावती दिखेगी, उनमें लक्ष्मीबाई दिखेगी, उनमें भारत माता दिखेगी। इसमें कोई संदेह नहीं कि उनके आँचल में बंध कर ही यह सभ्यता अगले हजारों वर्षों का सफर तय कर लेगी। छठ डूबते सूर्य की आराधना का पर्व है। डूबता सूर्य इतिहास होता है, और कोई भी सभ्यता तभी दीर्घजीवी होती है जब वह अपने इतिहास को पूजे। अपने इतिहास के समस्त योद्धाओं को पूजे और इतिहास में अपने विरुद्ध हुए सारे आक्रमणों और षड्यंत्रों को याद रखे। छठ उगते सूर्य की आराधना का पर्व है। उगता सूर्य भविष्य होता है, और किसी भी सभ्यता के यशश्वी होने के लिए आवश्यक है कि वह अपने भविष्य को पूजा जैसी श्रद्धा और निष्ठा से सँवारे... हमारी आज की पीढ़ी यही करने में चूक रही है, पर उसे यह करना ही होगा...
यही छठ व्रत का मूल भाव है। मैं खुश होता हूँ घाट जाती स्त्रियों को देख कर, मैं खुश होता हूँ उनके लिए राह बुहारते पुरुषों को देख कर, मैं खुश होता हूँ उत्साह में सराबोर बच्चों को देख कर... सच पूछिए तो यह मेरी खुशी नहीं, मेरी मिट्टी, मेरे देश, मेरी सभ्यता की खुशी है। मेरे देश की माताओं!जब आदित्य आपकी सिपुलि में उतरें, तो उनसे कहिएगा कि इस देश, इस संस्कृति पर अपनी कृपा बनाये रखें, ताकि हजारों वर्ष बाद भी हमारी पुत्रवधुएँ यूँ ही सज-धज कर गंगा के जल में खड़ी हों और कहें- "उगs हो सुरुज देव, भइले अरघ के बेर..."
जय हो…. जय छठी मईया….💐💐💐💐💐 छठ महापर्व की हार्दिक, अनेकानेक शुभकामनाएं।
आप सभी मेरे साथ जुड़ सकते हैं नीचे दिए गए लिंक पर जाकर और अपने विचार रख सकते हैं। धन्यवाद 🙏
Although the first thought in a football player with acute chest pain is usually towards cardiac causes, there are a number of life-threatening, non-cardiac, conditions that present with acute chest pain that need to be considered. It should be noted that football players with a potentially life-threatening cause of chest pain may appear initially relatively well, showing neither vital sign nor physical examination abnormalities. However, whatever the source of the chest pain may be, healthcare providers should always focus on the immediate detection of common life-threatening causes of chest pain and treat accordingly.
Primarily, “non-cardiac” causes of acute chest pain can to be differentiated by the origin of the pathology. Some of these non-traumatic, non-cardiac life-threatening medical emergencies are listed below and are included mainly for information and completeness.
Acute aortic dissection:-
The most critical cause of severe aortic-type chest pain is acute aortic dissection. In a football player, this would usually be due to congenital abnormalities, hypertension or connective tissue disease. One example would be a dissection which occurs in a player with Marfan syndrome. The event that may precede a fatal tear or dissection may be due to simple blunt trauma to the chest.
Acute pulmonary embolism:-
Although pulmonary embolism (PE) is thought to be a rare life-threatening field-of-play medical emergency, the exact incidence is unknown. However, its existence is always possible because of the frequent travel, that may increase the risk of PE above that of normal.
Exercise-induced bronchospasm:-
While shortness of breath and wheezing are more common symptoms associated with exercise-induced bronchospasm (EIB), players may also experience chest pain. This diagnosis is considered in more detail in the respiratory module.
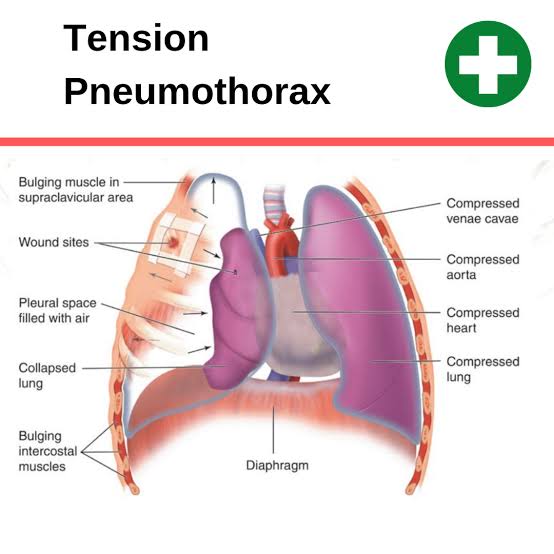
Tension pneumothorax:-
A tension pneumothorax is a medical emergency. In a football setting, it is frequently associated with a rib fracture. The presentation and management of this condition is considered in more detail with “chest injuries” later in this module.
Inflammatory or infectious:-
Pleuritis, pneumonia, bronchitis and mediastinitis are rare on the field of play because signs and symptoms would have presented prior to the match or competition.
Treatment
Player should be removed from the field of play and advised against further physical exercise. They may require analgesia or antipyretic drug therapy. They should be treated symptomatically and transferred urgently to the nearest, most appropriate medical facility if clinically unstable.
Acute gastrointestinal conditions:-
As the cardiac system and the oesophagus share some common neurologic innervations, acute pathology in either system can present with classical symptoms of chest tightness, provocation by exercise and pain-release by rest or nitrates.
As such, it may be difficult to distinguish clinically between cardiac chest pain and pain originating from the gastrointestinal system. Common, or more significant, gastrointestinal conditions include gastro-oesophageal reflux, oesophageal spasm, oesophagitis and spontaneous oesophageal rupture.
Symptoms and signs
Players with gastrointestinal conditions may experience chest pain, painful swallowing, tachypnoea or dyspnoea. Cyanosis, fever and shock may develop rapidly when there is a more significant problem.
Treatment
The player should be removed from the field of play and advised against further physical exercise. One should obtain intravenous access and administer fluids as required. The player should otherwise be treated symptomatically and, if clinically unstable, transferred urgently to the nearest, most appropriate medical facility.
Thank you for reading, Stay tuned. Keep supporting given below links.
Blue Tigers defender Adil Khan feels Indian Football is moving forward and growing on “the right path” that corroborates its new motto – “Indian Football. Forward Together”.
“Indian Football is growing in a good way and through the correct path. I just wish (Indian football) keeps growing the way it has been and tries to maintain the quality,” the 32-year-old defender expressed during an AIFF TV interview, a year after he faced off with neighbours Bangladesh at the Salt Lake Stadium, Kolkata.
He praised the authorities for resuming football actions in the country in the aftermath of the Lockdown that was enforced owing to the COVID-19 pandemic.
“It is great! After more than seven months without any football activity, we’re back to the pitch once again. I followed the Hero I-League Qualifiers closely and have noticed the positive buzz around it – that’s fantastic. Kudos to the AIFF for bringing back sports, let alone football, move one step closer to normalcy.”
He further added, “It was difficult for everyone who is connected to football – supporters, owners, players and every single stakeholder. Our pre-season has also started. I am very excited and hopefully, everyone is.”
Following an aggravated injury that had halted his footballing career, Adil came back strongly to appear for the Blue Tigers after a seven-year hiatus. The sturdy central defender lauded the changes that have been brought into Indian Football to move things ahead, as players can now avail better infrastructure.”During my initial days, there was a dearth of quality grounds. Infrastructures, facilities have improved immensely since then. These things always help a player perform to their true potential. That has helped Indian players perform in a better way,” stated Adil.
“Earlier, teams used to depend heavily on foreigners to churn out results. But, the scenario has changed of late. Indians have been taking responsibilities and proving their worth. They are scoring goals, providing assists, taking guards in the defensive half, tackling with more conviction – only to take Indian Football forward,” the 32-year-old opined.
आप सभी मेरे साथ जुड़ सकते हैं नीचे दिए गए लिंक पर जाकर और अपने विचार रख सकते हैं। धन्यवाद 🙏
अच्छा कोच या गुरु कैसा हो? ऐसा जोकि अपने विद्यार्थियों को प्यार दुलार से समझाए या ऐसा जोकि ज़रूरत पड़ने पर विद्यार्थियों और खिलाड़ियों पर लात घूँसे बरसाए, गालियाँ दे! आज की शिक्षा पद्वति के हिसाब से शिक्षक यदि किसी छात्र-छात्रा पर ज़रा हाथ उठा दे तो उसकी नौकरी ख़तरे में पड़ जाती है। इसी प्रकार यदि कोच अपने किसी खिलाड़ी को डाँट दे तो उसकी खैर नहीं। लेकिन भारतीय महिला हॉकी में एक ऐसा कोच हुआ है, जिसने पुरुष खिलाड़ियों के साथ साथ महिला खिलाड़ियों को भी जमकर पीटा, गालियाँ दीं और ज़रूरत पड़ने पर सरे राह उन पर हाकियाँ भी बरसाईं।
यह बदमिज़ाज और बदतमीज़ कोच बलदेव सिंह है, जिसने भारतीय महिला हॉकी को 80 के लगभग अंतरराष्ट्रीय खिलाड़ियों से सुसज्जित किया, जिनमें से सात ने भारत की कप्तानी की। वर्तमान कप्तान रानी रामपाल, नवजोत, नवनीत, मोनिका, रीथ, मनप्रीत आदि लड़कियाँ भी उसकी शिष्या हैं। ऐसे सिरफिरे कोच को जब 2009 में द्रोणाचार्य सम्मान मिला तो जलने वाले खूब जले। लेकिन ज़्यादातर ने कहा,”कोच हो तो बलदेव जैसा”।
हॉकी प्रेमी जानते हैं कि हॉकी जगत में नेहरू हॉकी टूर्नामेंट सोसाइटी का नाम बड़े आदर के साथ लिया जाता है। 1964 में पहले सीनियर नेहरू टूर्नामेंट की शुरुआत हुई थी लेकिन तीस साल बाद जब बालिकाओं के अंडर 17 टूर्नामेंट का बिगुल बजा तो इसे भारतीय महिला हॉकी में एक नई क्रांति की शुरुआत माना गया। जिस हरियाणा की लड़कियों को आज कुश्ती और मुक्केबाज़ी में अव्वल माना जाता है, उसकी लड़कियों ने मान सम्मान कमाने की दिशा में बड़ा कदम हॉकी खेल कर बहुत पहले उठा लिया था।
जहाँ तक हरियाणा में हॉकी क्रांति की बात है तो शुरुआत शाहबाद मार्कंडा के श्री गुरु नानक प्रीतम गर्ल्स स्कूल से हुई। साई कोच बलदेव सिंह ने गन्ना मजदूरों, रेहड़ी पटरी लगाने वालों, रिक्शा और ऑटो रिक्शा चलाने वालों की बेटियों को हॉकी सीखाने का जिम्मा उठाया। दो साल बाद जब 1994 में शाहबाद स्कूल की लड़कियाँ शिवाजी स्टेडियम में नेहरू बालिका टूर्नामेंट में खेलने उतरीं तो किसी ने सोचा नहीं था कि सिर पर चुनरी ओढ़ने वाली लड़कियाँ राँची, राउरकेला, दिल्ली, पंजाब, चंडीगढ़, लखनउ की टीमों को हराते हुए फाइनल में जा चढ़ेंगी।
अंततः ख़िताबी मुक़ाबले में राँची के स्कूल से हार कर उपविजेता बनीं। कोच बलदेव ने मीडिया के सामने अपनी टीम की लड़कियों को भद्दी गलियाँ दीं, जिन्हें सुनकर हॉकी प्रेमी हैरान थे। इतने से भी दिल नहीं भरा तो कोच ने तालकटोरा स्टेडियम से सटे पुलिस अधिकारी किरण बेदी के निवास के समीप अपनी कुछ लड़कियों की हॉकी स्टिक से पिटाई कर डाली। तमाशा देख रहे आम लोगों ने बलदेव को बुरा भला कहा। उन पर केस करने की भी बात चली।
बलदेव का यह रूप देख कर मीडिया भी हैरान था। नेहरू सोसाइटी के सचिव शिव कुमार वर्मा और डाक्टर केजी कक्कर से सवाल जवाब हुए लेकिन कोच ने माफी नहीं माँगी। बलदेव के तेवर देख कर क्लीन बोल्ड का कौतूहल जाग गया, शाहबाद स्कूल स्थित साई अकादमी का दौरा तय हुआ। वहाँ जाकर देखा कि शाहबाद की लड़कियाँ लड़कों की टीम से मुकाबला कर रही थीं।
चूँकि मुकाबला बराबरी पर ख़त्म हुआ, इसलिए बलदेव अपनी लड़कियों को उनके माँ-बाप की मौजूदगी में हॉकी से पीट रहे थे। खूब गलियाँ भी दे रहे थे। लेकिन किसी को भी कोच के रवैये से एतराज नहीं था। कुछ ग़रीब अभिभावकों के अनुसार कोच साहब उनके परिवारों के लिए भगवान का अवतार बन कर आए थे। साई से सेवानिवृत होने के बाद वह फतेहगढ़ साहिब में खिलाड़ियों की फ़ौजें तैयार कर रहे हैं। शाहबाद के बाद अब उन्होने फ़तहगढ़ साहिब और अमृतसर को महिला हॉकी का गढ़ बना लिया है।
1997 में शाहबाद ने पहली बार नेहरू बालिका खिताब जीत कर अपने विजय यात्रा की शुरुआत की। 16 बार विजेता, चार बार उपविजेता, तीन बार ख़िताबी तिकड़ी बनाई। बलदेव को बार बार श्रेष्ठ कोच आँका गया। इसके साथ ही हरियाणा ने राष्ट्रीय हॉकी में भी मजबूत कदम रखा। सालों साल हरियाणा और रेलवे के बीच राष्ट्रीय हॉकी के फाइनल खेले गए। रेलवे का पलड़ा इसलिए भारी पड़ता क्योंकि बलदेव की शाहबाद अकादमी की तमाम खिलाड़ियों को रेलवे ने अपने बेड़े में शामिल कर लिया था। इतना सब होने के बावजूद भी उसने गाली देने और खिलाड़ियों को सरे आम पीटने का सिलसिला जारी रखा।
यह बलदेव की गालियों का ही चमत्कार है कि उनके द्वारा तैयार खिलाड़ी भारतीय रेलवे और अन्य विभागों में उच्च पदों पर हैं, हज़ारों लाखों कमा रही हैं, देश के बड़े से बड़े खेल सम्मान पा रही हैं और उनके माता पिता कहते हैं कि जो कुछ पाया, सर की गालियों से मिला है।जब वह गाली नहीं देते, बेटियों को हॉकी से नहीं पीटते, बहुत बुरा लगता है। ऐसा प्रतीत होता है जैसे हम से नाराज़ हों।
🗣️ आप सभी मेरे साथ जुड़ सकते हैं नीचे दिए गए लिंक पर जाकर और अपने विचार रख सकते हैं। धन्यवाद 🙏
Chest injuries in football are almost exclusively limited to chest wall muscle tears and fractured ribs, when such rare events do occur. The mechanism of injury for fractured ribs is contact against a hard object. Common injury mechanisms include a direct blow from an opponents elbow, a hard landing onto the field of play or collision against the goalposts. Whatever the mechanism of chest wall injury, most injuries cause severe pain, and removal from the field of play is usually warranted, either temporarily or for the duration of the match, unless the chest wall can be adequately strapped to alleviate the pain and allow functionality once again.
Chest trauma
Chest trauma most commonly occurs after a direct blow – most often with an opponent.
Two type :- Rib Feature & tension pneumothorax
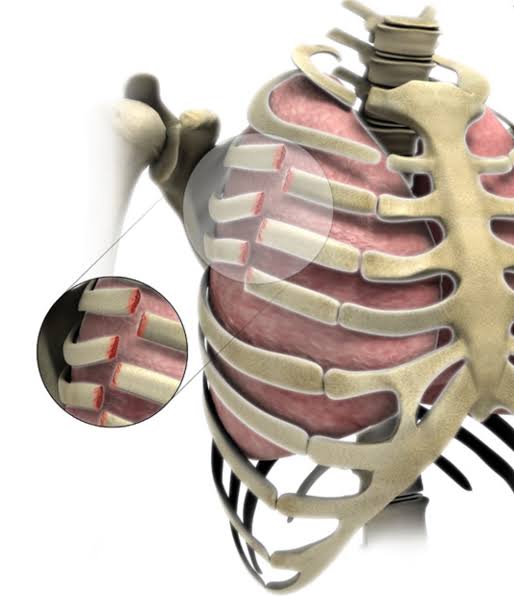
1. Rib fractures
Rib fractures are the most common injury sustained following blunt chest trauma. They account for more than 50% of all thoracic injuries from non-penetrating trauma. Approximately 10% of all patients admitted after blunt chest trauma have one or more rib fractures. These fractures are rarely life threatening but can be a sign of a more severe visceral injury inside the abdomen and the chest. Fractures generally occur at the site of impact or the postero-lateral bend, where the rib is weakest.
History:-
Patients who have fractured a rib/ribs typically present with significant pain related to the affected area. They often have pain with breathing (particularly inspiration).
Examination:-
The typical signs of a rib fracture include visible distress, pain on manual compression of the rib(s) over the affected site and the presence of bruising or swelling over the fracture site. It is very important to consider the possibility of a more significant injury. Assess the player post injury for alertness, adequacy of the airway, breathing and circulation status. You should also assess the lung breath sounds bilaterally to ascertain if a clinical pneumothorax is present.
A fractured rib may tear the visceral pleura and underlying lung and cause a pneumothorax. This may not be clinically detected if small – or it may be larger and present clinically with decreased breath sounds found on auscultation and increased resonance on percussion on the affected side. Should this occur, a decision must be made regarding management of the pneumothorax, if at all.
Investigation:-
In some situations, rib fractures are not well demonstrated on x-ray images. When an x-ray appears normal, but there are clinical signs suggestive of a fracture, the player should generally be treated symptomatically – rather than pursuing further imaging. A chest x-ray series can generally demonstrate a pneumothorax well. CT imaging is generally the next best study. Monitoring pulse oximetry or checking arterial blood gases may be required when there is a pneumothorax.
Treatment:-
Uncomplicated rib fractures can generally be managed symptomatically. The player may be allowed to continue as long as they are comfortable. Analgesics and chest wall strapping may provide some assistance. These injuries are generally very painful and usually prevent players from returning to competitive football for four to six weeks. If there are signs of a pneumothorax, or other associated internal organ injury, then the player should be urgently transferred to the nearest, most appropriate medical facility, with the addition of supplemental oxygen via face mask during ambulance transfer.
Pneumothoraces can be treated with observation (when small), aspiration and small-bore catheter insertion. These treatments are effective, take less time and have fewer complications when compared with inserting a chest drain.
2. Tension pneumothorax
If the fractured rib(s) have resulted in a clinical pneumothorax with deteriorating symptoms and signs, the presence of a tension pneumothorax must be considered, clinically sought and, if present or in any doubt, requires urgent treatment. This rare but life-threatening medical emergency is caused by a tear in the lung airways, such that during inspiration, air escapes into the pleural space, while during expiration the air is trapped inside the pleural space, due to a valve-like mechanism. This results in successive volumes of air entering the pleural space slowly compressing the unilateral affected lung, then compressing the mediastinum until the heart itself is pushed to the opposite side from the increasing pleural pressure. Once the heart is moved, compression and closure of the superior and inferior vena cavae may occur, decreasing venous return to the right side of the heart and thereby decreasing cardiac output, leading to severe hypovolaemic shock and eventually non-output cardiac arrest.
History:-
Any player who appears short of breath or tachycardic at rest (following chest trauma) should be assumed to have a tension pneumothorax. Signs of shock should also be taken very seriously.
Examination:-
In addition to signs suggesting shock following a chest injury, the following findings should prompt a diagnosis of a tension pneumothorax.
Decreased or absent breath sounds on the affected side
Hyper-resonance to digital percussion on the affected side
Distended neck veins
Displacement of the cardiac apex beat to the non-affected side
Deviation of the trachea to the non-affected side
InvestigationsIf there is clinical evidence or even a suspicion of a tension pneumothorax being present from the clinical picture of the patient, immediate treatment must be undertaken to decrease the pressure within the affected pleural space.
One must never refer the patient for radiological investigation in order to confirm the diagnosis, because this may lead to cardiac arrest from delayed release of life-threatening intra-pleural pressure. Tension pneumothorax is always a clinical diagnosis and should never be seen on a radiological investigation.
Emergency treatment:-
Treatment of a tension pneumothorax is aimed at immediately decreasing the raised intra-pleural pressure, thus allowing the displaced heart to return to its original position with opening of the superior and inferior vena cavae, and thus restoration of venous return and hence cardiac output. This is achieved by making a hole in the chest wall into the pleural cavity and thus releasing the entrapped gas under pressure. This can be undertaken by inserting a standard 5-cm long, large bore (16G / 14G) intravenous catheter needle. This should be done into the affected pleural cavity in the fourth or fifth intercostal space, immediately above the rib perpendicular to the skin, in the vicinity of the anterior or mid axillary line. This location is selected because the thickness of the chest wall at the anterior mid axillary line is 1 cm thinner than that at the traditional second intercostal space, mid-clavicular line.
Follow these steps to successfully manage a tension pneumothorax.
Place the player in either a lateral recumbent position with the affected side up, or supine, with the head of the bed up 40-45 degrees.
Identify the fourth or fifth intercostal space in the anterior axillary line.
Prep the area.
Insert the 14- or 16-gauge catheter needle just above the rib, perpendicular to the skin. As you traverse the pleura, you may hear the distinctive rush of air from the decompressed tension pneumothorax.
Remove the needle and leave the catheter in place, securing it to prevent dislodgment.
Re-evaluate the patient to ensure a positive clinical effect and continue to monitor the patient closely as you complete the evaluation and resuscitation.
Treat the residual “simple pneumothorax”
Although air may escape under pressure from the catheter, these are known to kink or displace fairly easily, and therefore the patient must be constantly monitored until safe arrival in an emergency department where radiological investigations can be undertaken to determine the exact diagnosis, and be treated accordingly.
Thank you for reading, keep supporting given below links.
While the regulated lifestyle and rigorous training regimes of footballers – who work diligently to improve fitness in the gyms, follow stringent diet plans, study various tactics to function as a team – is well known, what often tends to escape our attention is the equally intense behind-the-scenes preparation, undertaken by match officials to ensure the game is enjoyed on a truly level playing field.
In an exclusive chat on AIFF TV, eminent referee Rowan Arumughan opened up about the crucial role that meditation plays in his pre-match routine.
“Meditation is a part of preparation. It helps the referees focus and improve concentration. However, there are many other aspects too,” said the FIFA panel referee, before going on to detail the four points that he believes are crucial for every referee to make the cut at the very top level of the sport.
“Fitness is first,” he enumerated. “A Ref has to maintain fitness throughout the year, there is no off season. At any given time, he has to be ready for a fitness test. If a person is not fit but has all the knowledge – what is the use of putting him on the field of play? No one will accept that.”
“Knowledge of the ‘Laws Of The Game’ is also of paramount importance. If the referee is fit but not aware of laws then again there’s no use of putting him out there,” continued the referee who in 2011 was picked to officiate in Lionel Messi’s first game as captain of Argentina as they went up against Venezuela in a FIFA friendly at the Vivekananda Yuba Bharati Krirangan in Kolkata.
“Another very important thing is teamwork. When we go to officiate, along with the assistant referees and fourth official, we all work as a team, to come through a situation successfully. Without the team we cannot succeed in any aspect.” stressed Rowan.
“Information about teams and players also becomes important while reading a game,” he explained how referees need to have adequate information about the players in every game. “They should know about the players who are skilful. These are the players who can challenge the referees.”
“All of these combined, we also need to be consistent, if you do well in one match and not in the next, it doesn’t work. You need to perform consistently over time to gain respect. When you gain respect, players understand and know that this referee minds his own business, so that makes life easier,” he stated.
Thank you for reading , keep supporting given below link.
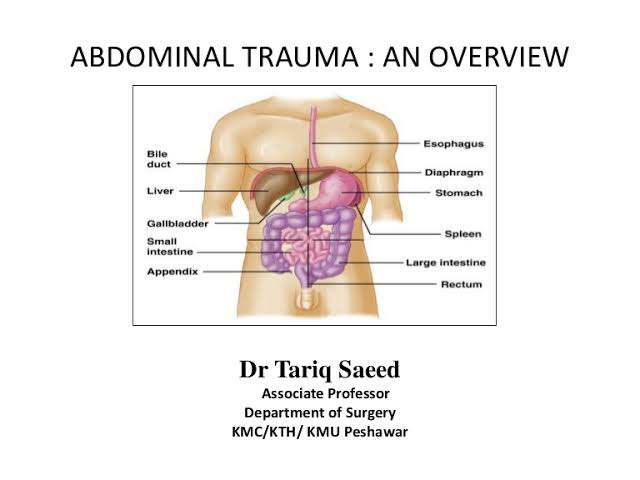
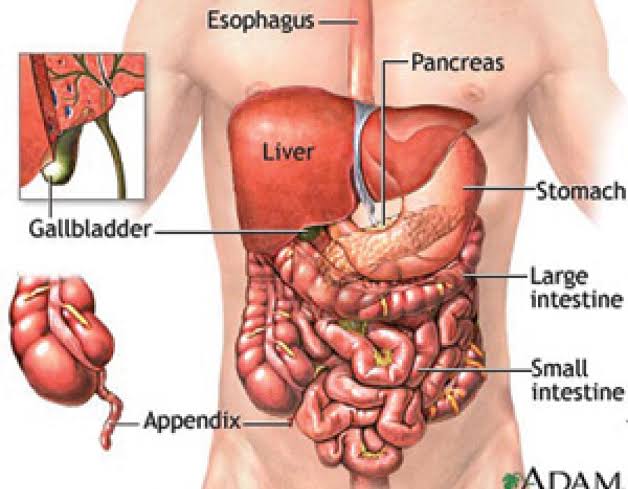
Abdominal injuries in football are an uncommon event; however, they appear to be happening more frequently. Abdominal injuries do not present as obviously as many orthopaedic injuries, because of the internal and concealed locations of the intra-abdominal organs. A high index of suspicion and knowledge of the mechanism of injury may contribute to the earlier diagnosis of acute, serious abdominal injuries.
Blunt trauma to the abdomen may cause injury to the solid organs of the abdomen, namely the liver, spleen or possibly a kidney, resulting in intra-abdominal haemorrhaging.
This can potentially be life threatening, depending on the extent of the haemorrhage. The injured player may present with relatively modest pain initially and over time develop hypovolaemic shock as the haemorrhage increases. The hollow organs (e.g. the jejunum colon and duodenum) can also be injured.
History:-
Pain may occur after an abdominal injury, but this does not always occur. Pain may not occur until signs of peritonitis develop hours after the injury.
Examination:-
The traditional examination of the abdomen, including inspection, palpation, percussion and auscultation, may reveal bruising, tenderness, guarding and loss of bowel sounds. The player should be assessed for evidence of shock, although signs can develop over time. This is especially common following the rupture of a hollow organ. Serial physical examinations have been shown to be a sensitive way to detect early intra-abdominal haemorrhage and are a practical way to assess these players.
Investigations:-
In general terms, any player who is suspected of having an injury to an intra-abdominal organ should have a CT scan. Ultrasound scans, including FAST scans, can be a helpful initial study. X-rays are not generally useful but may show pneumoperitoneum or obliteration of the psoas shadow (when there is a retroperitoneal haematoma). Baseline blood tests, including a cross match, should be taken. It is important to especially consider the patient’s haemoglobin.
A mid-stream urine test is also useful when an injury to the genitourinary tract is suspected.
Treatment:-
Injured players in hypovolaemic shock are managed like any other patient in shock with protection of the airway, supplemental oxygen administration, if present, intravenous access and limited crystalloid administration sufficient to maintain a blood pressure at 90mmHg and an appropriate diluted, titrated infusion of an intravenous analgesia with emergent transfer to hospital. Hypotensive resuscitation is preferred in such patients, because injudicious use of large quantities of intravenous crystalloids may result in increasing the blood pressure at the bleeding site and worsen the bleeding. Therefore, the sooner the player is transferred to hospital and under the care of a surgeon the better.
Once a diagnosis has been made, a decision must be made about whether the injury requires surgical management. In many cases, liver and spleen injuries can be managed non-surgically.
Thank you for reading. Keep supporting given below links.
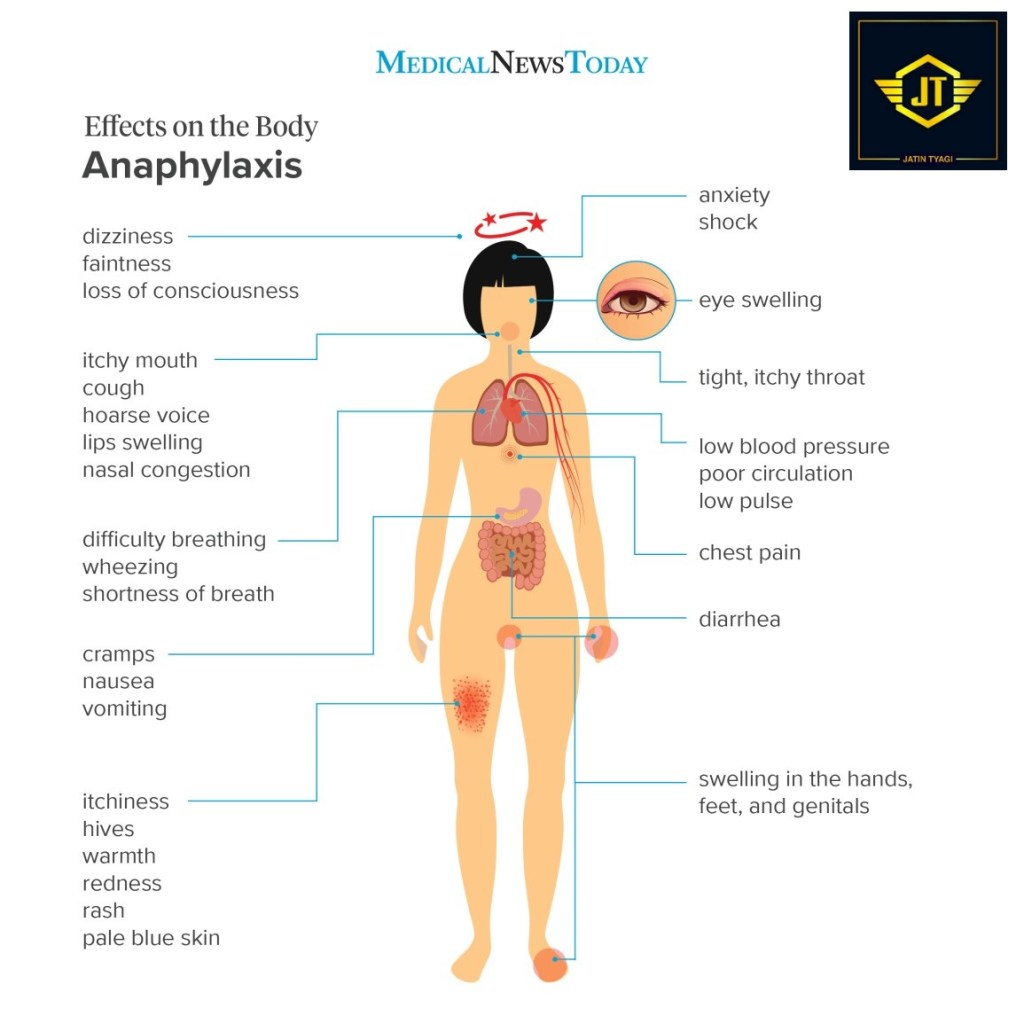
Severe anaphylaxis is an acute life-threatening allergic reaction. The risk of anaphylaxis in the football environment, both on and off the field of play, needs to be appreciated. Known trigger factors include food, medications, hymenoptera stings, fever and infections (such as upper respiratory tract infection). The risk of anaphylaxis may also be increased by “cofactors” that include non-steroidal anti-inflammatory medications (NSAIDS), exercise and alcohol. All of these precipitants may be relevant to the football environment. Travel into unfamiliar environments, particularly with regard to the consumption of food and drink, may increase the risk of severe allergic reactions.
The ability to recognise and manage anaphylaxis must be within the scope of team doctors and football stadium medical services.
History and examination
Prompt recognition and immediate treatment is essential in anaphylaxis. The following clinical criteria, adapted from the World Allergy Organisation Guidelines, are relevant within the football environment.1-3
Anaphylaxis must be considered when any one of the following clinical criteria is present:
Acute onset of illness involving the skin, mucosal tissue or both (e.g. general urticaria, itching, redness, swollen lips, tongue or uvula)
Gastrointestinal – severe cramps, abdominal pain, vomiting
OR
Reduced blood pressure after known or possible exposure to a likely allergen:
Children – low systolic blood pressure or greater than 30% decrease from normal for age.
Adults – systolic blood pressure less than 90mmHg or greater than 30% decrease from normal for the person.
Treatment
The key to the successful treatment of severe anaphylaxis in the football environment is early identification, an appreciation of its life-threatening consequences and initiating immediate treatment with adrenaline/epinephrine.
In any situation where any of the above clinical signs or symptoms occur in the context of a possible allergic reaction to food, medications, hymenoptera stings (e.g. bees) or other chemicals, always consider the possibility of anaphylaxis immediately. It is always better to treat the player early rather than await clinical deterioration, as hesitation in the treatment of severe anaphylaxis can be fatal.
The mainstay of treatment of severe anaphylaxis is the administration of epinephrine (adrenaline) by intramuscular administration into the antero-lateral thigh (vastus lateralis).
Epinephrine(adrenaline):-
If an auto-injector (e.g. an EpiPen™) is available, it is used by thrusting the device appropriately against the antero-lateral thigh. This can be done through clothing if necessary. The pen should be held against the thigh for at least 10 seconds to allow full intramuscular injection of the intended epinephrine dose (0.3mg in an adult injector or 0.15mg in a child injector).
If epinephrine is only available in ampoule form as a 1:1000 (1mg/ml) concentration (or repeated doses of epinephrine are required without an additional auto-injector being available), administer 0.5mg (equal to 0.5ml of the 1:1000 epinephrine) intramuscularly (IM) into the antero-lateral thigh in an adult or 0.3mg in a child. Before injecting the epinephrine into the thigh muscle, withdraw the syringe plunger to ensure that the needle is not in a vein, as intravenous concentrated Epinephrine injection can have serious cardiac effects.
If severe symptoms continue after epinephrine IM injection, repeat the dose every five minutes. An ambulance should be called (if not already on site).
If, after epinephrine administration, the patient remains hypotensive (i.e. there is no radial pulse), position the patient supine and elevate the legs. Establish intravenous access as soon as practically possible and consider administering normal saline, or equivalent solution, in order to obtain a systolic blood pressure of 90mmHg minimum. Colloids may be considered, although there is no evidence to substantiate their use. Note that up to 50% of the intravascular volume can be lost within ten minutes in severe anaphylaxis, thus initially requiring potentially large volume replacement.
Beta-2 agonists:-
In the presence of anaphylactic-induced bronchospasm, in addition to epinephrine administration, consider the use of β2-agonist inhalation, either by an inhaler and spacer or via oxygen-powered nebulisation. This treatment can be repeated as often as necessary.
Antihistamines:-
There is no evidence that the administration of antihistamines in severe anaphylaxis has any beneficial effect in the initial management. As a result, it is not suggested as part of the immediate response. Once the patient has been transferred to the nearest, most appropriate emergency department, the use of an antihistamine can be considered after a full medical history and examination has been undertaken, possibly for the relief of urticaria and itching symptoms.
Glucocorticoids:-
There is no evidence that the administration of glucocorticoid medications in severe anaphylaxis has any beneficial effect in the initial management. As a result, it is not suggested as part of the immediate response. Its administration, once the patient has been transferred to the nearest, most appropriate emergency department, can be considered after a full medical history and examination has been undertaken.
The patient should be transferred to the nearest, most appropriate medical facility as soon as possible after the initial dose of epinephrine/adrenaline has been administered, so that further support may be administered by the emergency department, if and when necessary.
Follow-up
Discharge follow-up and educational strategies to prevent further occurrences and treat possible future events may be required from sports healthcare professionals overseeing the healthcare of the team member, where relevant.
Thank you for reading, stay tuned. Keep supporting given below links.
हाल ही में एथलेटिक फेडरेशन के अध्यक्ष आदिल सुमरीवाला ने एक बयान में कहा कि भारत ओलंपिक में स्वर्ण पदक जीत सकता है। उनके बयान पर देश के एथलेटिक जानकारों और पूर्व चैंपियनों के कान खड़े होना स्वाभाविक है। सभी एक दूसरे से पूछ रहे हैं कि भला ऐसा कौनसा एथलीट है जिससे ओलंपिक स्वर्ण की उम्मीद की जा रही है!
संभवतया फ़ेडेरेशन अध्यक्ष को लगता है कि भारत को अपना पहला ओलंपिक स्वर्ण आगामी टोक्यो ओलंपिक में मिल सकता है। फ़ेडेरेशन और मीडिया के एक वर्ग ने जिन एथलीटों को सबसे ज़्यादा भाव दिया है और जिनसे ओलंपिक पदक की उम्मीद व्यक्त की जा रही उनमे नीरज चोपड़ा, हिमा दास और दुति चन्द के नाम सबसे पहले लिए जाते हैं। इस कतार में कुछ रिले रेस भी शामिल की हैं। नीरज लंबे समय तक चोट से जूझने के बाद ट्रैक पर उतर आया है और उसने ओलंपिक टिकट भी पा लिया है। हिमा और दुति को पहले ओलंपिक के लिए क्वालीफ़ाई करना है तत्पश्चात ही पदक के बारे में सोच सकती हैं।
कोरोना वायरस के फैलाव के कुछ सप्ताह पहले तक हिमा और दुति ने यूरोपियन सर्किट में खूब धमाल मचाया था। एक के बाद एक कई दौड़ें जीत कर देशवासियों को गदगद कर दिया। मीडिये के कुछ लोग तो यहाँ तक कहने लगे थे कि भारत को ओलंपिक मैटेरियल मिल गया है। आख़िर जब पूरा जोड़ घटा कर देखा गया तो दोनों महिला एथलीटों के प्रदर्शन को खारिज कर दिया गया। अपने ही कुछ नामी कोच तो यहाँ तक कहने लगे कि यह प्रदर्शन सिर्फ़ छलावा है। कुछ एक के अनुसार ओलंपिक पदक के लिए उनकी तैयारी अभी नाकाफ़ी है और उनके पास ज़्यादा वक्त भी नहीं बचा है।
एथलेटिक अन्य खेलों की जननी मानी जाती है और चूँकि एथलेटिक में भारतीय प्रदर्शन अच्छा नहीं रहा इसलिए बाकी खेलों में भी छुट पुट कामयाबी मिल पाई है। लेकिन शर्म की बात यह है कि डेढ़ सौ करोड़ की आबादी अपने पहले ओलंपिक पदक के लिए छटपटा रही है। भले ही कितना झूठ बोलें दावा करें, अगले दो ओलंपिक तक भी ओलंपिक गोल्ड मिल पाना आसान नहीं लगता। हाँ कोई चमत्कार हो जाए तो बात अलग है।
हर ओलंपिक से पहले बहुत कुछ कहा सुना जाता रहा है और बड़ी बड़ी डींगें हांकी जाती हैं। भारी भरकम दल के लिए तिकड़म लड़ाई जाती हैं लेकिन बार बार और लगातार खाली हाथ और विवाद के साथ लौटने की परंपरा सी बन गई है। टोक्यो में यदि ओलंपिक आयोजन हुआ तो यही कहानी फिर दोहराई जाएगी। इस बार तो सहानुभूति के भी अच्छे ख़ासे नंबर मिल जाएँगे। खेल मंत्रालय को कोरोना के नाम पर घड़ियाली आँसू बहाकर भाव विभोर किया जा सकता है। अर्थात ओलंपिक पदक या गोल्ड जीतने के झाँसे के साथ टीम का आकार भी बड़ा किया जा सकता है। यह रणनीति कलमाडी काल से अपनाई जा रही है लेकिन तब भारतीय एथलीटों का प्रदर्शन कहीं बेहतर था।
जहाँ तक भारतीय एथलेटिक के श्रेष्ठ की बात है तो मिल्खा सिंह और पीटी उषा के प्रदर्शन पर हम भारतीय गर्व करते आए हैं। इसमें दो राय नहीं कि तमाम अंतरराष्ट्रीय मुकाबलों में दोनो भारतीय एथलीटों ने शानदार प्रदर्शन किया। ख़ासकर पीटी उषा अभूतपूर्व रहीं। एशियायई खेलों और एशियन चैंपियनशिप में उषा को मिली कामयाबी की कोई भारतीय खिलाड़ी बराबरी नहीं कर पाया। मिल्खा नें 1960 के रोम ओलंपिक में 400 मीटर दौड़ में और उषा ने 1984 के लास एंजेल्स ओलंपिक की 400 मीटर बाधा दौड़ में चौथा स्थान अर्जित किया। अंजू बाबी जार्ज, बीनामोल, शाइनी अब्राहम, श्रीराम सिंह, गोपाल सैनी, मोहिंदर गिल, गुरबचन रंधावा और कुछ अन्य ने पहचान बनाई लेकिन पदक जीतने वाला प्रदर्शन अभी तक देखने को नहीं मिल पाया है।
आप सभी मेरे साथ जुड़ सकते हैं नीचे दिए गए लिंक पर जाकर और अपने विचार रख सकते हैं। धन्यवाद 🙏
A total of 19 clubs have applied for National and AFC club licences for the 2020-21 season, out of which 8 are from I-League and 11 are from ISL. The result of National and AFC Club licensing applications for the 2020-21 season made by ISL clubs have been announced yesterday and they are as follows :
Mr. Jatin Tyagi (Director of Pankration Fitness Academy Private Limited, Football Coach, Educator)
FC Goa, ATK Mohun Bagan FC, Bengaluru FC, Jamshedpur FC, Chennaiyin FC and Mumbai City FC have successfully secured the AFC and National licences for the 2020-21 season.
Odisha Football Club, NorthEast United Football Club, Kerala Blasters Football Club, Hyderabad Football Club and Sporting Club East Bengal have failed to secure the AFC and National licences for the 2020-21 season. These clubs can now either prefer an Appeal to the Club Licensing Appeals Body of AIFF against the decision of the Club Licensing Committee – First Instance Body’s decision within the stipulated time or can apply for an Exemption to the Club Licensing Committee – First Instance Body’s decision within the stipulated time to participate in National Club Competitions in the 2020-21 season.
Owing to the current situation, the Asian Football Confederation have been considerate enough to accommodate criteria exception and deadline extension requests made by AIFF throughout the licensing cycle of 2020-21 season. As a result of it, many criteria were exempted from fulfilment and the deadline too were extended multiple times, with the Final deadline being 9th November 2020 for all 19 licence applicants of the 2020-21 season.
Due to paucity of time along with the no. of licensing reports up for evaluation and owing to the league schedule of the ISL, the Club Licensing Committee – First Instance Body have delivered their decision for ISL clubs only for now. The decision on the club licensing application of 8 I-League clubs will be taken soon.
All football players with a suspected or clinically symptomatic spinal injury must be adequately and appropriately stabilised to prevent neurological injury to the spinal cord or further injury. This means that all healthcare staff on duty should be fully trained in the recognition, evaluation, treatment, stabilisation and transfer of the head and/or neck injured player. The correct equipment must also be available (rigid spinal board, scoop stretcher or Stokes-type basket stretcher or vacuum mattress).
Please note that use of the traditional “NATO”-type soft stretcher is no longer acceptable on the field of play. A hard cervical collar is also no longer recommended.
The basic principles of spinal column stabilisation comprise the following actions:
Carefully, gently and slowly, realign the head into the neutral position relative to the spine and maintain this position thereafter. If this slow, gentle realignment causes any neck or spinal pain, muscle spasm, abnormal neurological signs or symptoms, offers resistance or compromises the integrity of the airway, then immobilise the head in the position found and transfer as such to hospital on an appropriate stabilisation device at hand.
Once the head has been adequately realigned and stabilised, carefully, gently and slowly align the entire spinal column into the neutral position, following the same principles as stated above.
If the player is lying on their back (supine), the player needs to be stabilised on a long, rigid, spinal-type board (RSB). This may be undertaken by a careful, gentle and coordinated log-roll manoeuvre to turn the player onto their side, placing the RSB behind the player’s back and then performing a careful, gentle coordinated log-roll to move the player onto the RSB in the supine position for stabilisation. Alternatively, the player may carefully, gently and with coordination be lifted off the ground by a team straddling the player while an RSB is slipped under the player, who is then gently lowered onto the RSB.
All players strapped to a stabilisation device should be strapped sufficiently securely so that the device can be urgently turned into the lateral position if the player vomits, without creating excess movement of the spine as a result.
If the player is lying on their side (lateral), an RSB can be positioned behind the player’s back and the player is then carefully, gently log-rolled onto the RSB into the supine position for stabilisation.
If the player is lying face down (prone), a number of careful, gentle coordinated steps are required by the medical team to first realign the head into the neutral position, then log-roll the player onto his/her side, and finally log-roll the player onto a RSB into the supine position for stabilisation.
Once the player has been adequately and appropriately aligned in the supine position, anatomically neutral onto an stabilisation device, manual cervical spinal stabilisation should be converted into external stabilisation using external devices (e.g. foam-based head blocks).
Thank you for reading, keep supporting given link below.
The management of significant trauma or medical conditions is complex and beyond the scope of this module. It is essential that a team doctor, stadium doctor or other clinicians working in football have a clear process for the assessment of medical and trauma emergencies. Having the appropriate equipment on site is also essential. The FIFA Medical Emergency Bag contains the equipment needed to manage the more common medical and trauma emergencies which might occur on the field of play.
It is always important to make sure that you have help. As soon as you suspect that you are dealing with a more significant problem, your first action should be to call for help. This usually means calling an ambulance if there are no other healthcare providers on site.
A basic approach involving a “primary survey” is outlined below. This involves treating the greatest threat to life first. The lack of a definitive diagnosis should not delay the treatment of life (or limb) threatening conditions.
Safety:-
An important part of the administration of any medical support is the safety of all people involved. The first active role of the clinician is to ensure their own safety and then the safety of the persons who require treatment. If the field is not safe to enter, for whatever reason, do not enter the field until it has been declared safe by the referee or local security personnel.
The risks on any football field are going to be reasonably well controlled. It is always worth taking a few seconds to make sure the area is safe and, if necessary, stop the match or training session while first aid treatment is carried out.
Safety issues specific to a football pitch include:
Other players – there may be arguments going on among opposing team players
Spectators – pitch invasion by spectators, throwing of missiles onto the field of play
Unsuitable pitch conditions – uneven or slippery surfaces
Adverse weather conditions – e.g. lightning
It is also important to protect yourself from potentially contaminated body fluids. Use gloves and consider the use of eye protection and other protective clothing. The FIFA Medical Emergency Bag (FMEB) contains gloves and a pair of goggles.
Airway:-
The first stage of the assessment is to assess the player’s airway – with cervical spine protection. Look inside the player’s mouth to assess if anything is blocking their airway. Examples of items that may block a player’s airway on the field of play include the following:
A loose and poor fitting mouthguard
blood or vomit in the mouth
broken and loose teeth
mud (especially if the ground is wet and the player falls face down)
The airway can be opened by tilting the head backwards if there is no potential of a neck injury being present. If there is suspicion of a neck injury or trauma involved, then lift up the chin or do a jaw thrust. Any obvious obstructions should be removed if they are clearly visible and to the front of the mouth, use the Magill forceps from the FMEB. Do not place your fingers inside their mouth. If it is not possible to protect the airway using these simple manoeuvres, it may be necessary to insert an “airway adjunct” from the FMEB. If the player is on their side, you should leave them there until help arrives. If the player is prone, gently turn their head to the side enough to enable breathing. If the player is unconscious, they should be placed on their side (not their back).
The FIFA Emergency Medical Bag contains laryngeal masks, nasopharyngeal tubes and Guedel airways. There are also a ventilation bag and masks.
Breathing:-
Use a stethoscope to assess the player’s breathing. Remember that players who have suffered a sudden cardiac arrest may be breathing normally.
The aim of this assessment is to identify and manage six life-threatening thoracic conditions. These are: airway obstruction, tension pneumothorax, massive haemothorax, open pneumothorax, flail chest segment with pulmonary contusion and cardiac tamponade. Most of these conditions are rare in football.
If the player is breathing normally, continue with the assessment. If they are not breathing, CPR should be initiated.
Circulation:-
Look for and stop any external bleeding. Haemorrhage is the predominant cause of preventable post-injury deaths. If there is bleeding, applying direct pressure is the first response. Deep and firm direct pressure is applied to control the bleeding. Cover the area with your gloved hand and a (sterile) towel (if you have one).
One must also consider the possibility of internal bleeding. Tachycardia or reduced blood pressure may be the only sign of this.
The FIFA Medical Emergency Bag contains equipment to manage bleeding, including a variety of gauzes and tape for the compression of wounds. There is also a blood pressure cuff and stethoscope. An infusion set, tourniquet and IV lines are included and can be used to deliver IV fluids to support the player’s circulation.
Disability:-
A basic neurological assessment should be made, known by the mnemonic AVPU (alert, verbal stimuli response, painful stimuli response, or unresponsive). This is achieved by noting whether:
the player is fully alert and responsive to you
the player is not alert but is responsive to your voice
the player is not alert but does respond to your touch or to a painful stimulus e.g. earlobe squeeze
the player is totally unresponsive – does not respond to any of the above
Hypoglycaemia and drugs, including alcohol, may influence the level of consciousness. The FIFA Medical Emergency Bag includes a glucometer which can be used to assess blood glucose.
Exposure and examination:-
You cannot treat what you cannot see. You must be able to see the injury in order to be able to effectively treat it. Injuries may be hidden under the player’s clothing.
Expose the relevant injury by removing as much clothing as necessary to look for underlying injuries. You must also consider whether removing the players clothing is going to create more issues. For example, this may predispose them to becoming cold and developing hypothermia. It is also important to consider the player’s privacy.
Consider the player’s medical history that you are aware of so that you can pass this information on to the ambulance staff on arrival.
Once these steps have been completed, resuscitation efforts are underway and the player is stabilised (vital signs are normalising), a further evaluation (secondary survey) should be conducted. This involves a head-to-toe evaluation of the player, including a complete history and physical examination and a reassessment of all vital signs. In a football context, this can be done in the medical room or changing room before transfer to hospital. Each region of the body must be fully examined. During this phase, X-rays may be obtained. If at any time during the secondary survey the patient deteriorates, another ABCDE assessment must be carried out as a potential life threat may be present.
Thank you for reading, stay tuned!! Keep supporting given below link.
A number of relatively minor complaints can have a surprisingly large impact on a player’s ability to perform to their maximum potential. Many of these complaints can be effectively prevented through education, training or with minor treatments. It is important to develop an approach to managing these issues if you are going to be involved with a football team and provide touchline medical care.
Ear, nose and eye problems can be significant and have an impact on a player both in the short, medium and long term. While a clinician should be prepared to manage the more minor conditions, it is essential that they are able to identify the more significant issues and to seek further review when needed.
Thank you for reading. Keep supporting given link.
Here is a guideline to all aspiring new coaches and to already licensed football coaches who want to join the FUTSAL pathway.
Futsal is a specialized sport by itself and to coach a futsal team you need to get your AFC FUTSAL certification which is different from AFC Pro/A/B or AIFF C/D/C Football certificates.
Step 2. Once registered keep an eye out on your dashboard for upcoming courses on FUTSAL and apply for the same.
Step 3. Once your selection for the course is complete you will get a email from AIFF with the Fee and Schedule for the course applied.
Currently in India we have the AIFF Introductory Futsal Course Online. After completing this 3 day online course the next step is the AFC Futsal Level 1 Certificate Course which after successfully passing will you be qualified to give basic FUTSAL training for Grassroots.
Currently The Instructor with Futsal is Mr. Joshuah Vaz & Mr. Shailesh Karkera both are very kind , knowledgeable and the quality of course is very good ☑️
Only with correct knowledge and certified FUTSAL Coaches can we give correct training in FUTSAL to our grassroots.
Youth Futsal Academy which operates at Chowgule Sports Conditioning , Pankration Fitness Academy India (P.F.A INDIA) And Fitness Centre in Gogol Margao is currently the only FUTSAL academy in Goa with certified AFC Futsal Level 1 and Level 2 Coaches.
Come on over and JOIN us as we continue to develop better football players through FUTSAL .
Do Like and Share so that we can make FUTSAL big in INDIA very soon…
Thank you for reading, stay tuned. Keep supporting given below links.
There are a number of injuries that involve the ear that can occur during football. Some of these require prompt management to ensure that they do not cause ongoing deformity of dysfunction.
Cauliflower ear: This term refers to a haematoma between the skin and perichondrium (also known as traumatic auricular haematoma). If not treated appropriately, this type of injury can lead to lifelong deformity. The haematoma can become fibrotic within two weeks.
Initial treatment involves the use of ice and compression. Definitive treatment involves aspiration of the haematoma followed by direct compression with blue-tack/silicon or collodion-soaked gauze. To aspirate the haematoma, use a 20 gauge needle (or similar). After this has been done, the blue-tack should be used to attempt to preserve the normal shape of the ear. The player should then be examined daily to check their progress and to ensure that there has not been any recurrence. There is a small risk of infection with S.aureus or pseudomonas.
Otitis externa: This condition is common among those who swim or who train frequently in a pool. While it is generally caused by a bacterial infection, it can also be caused by a fungal infection. Players most commonly present with a painful and itchy ear. There may also be a discharge and in some cases impaired hearing.
On examination, the canal appears erythematous and a discharge may be observed. Tragal compression or tugging classically causes the player pain.
Treatment involves the player avoiding rubbing, scratching or Q-tips. Keeping the ear dry and the use of topical alcohol, oil or antibiotic drops are also generally useful strategies. Keeping one’s head above the water while in the pool is a good preventative strategy while topical alcohol applied after swimming, effectively dries the canal and prevents recurrence.
Tympanic membrane rupture: This typically happens after a direct blow to the ear or head. The player most commonly presents with pain, reduced hearing and sometimes bleeding. The player should be assessed with an otoscope to define and document the injury (and the size of the injury).
The majority heal with conservative management over two weeks. Treatment might involve the following:
try to avoid any topical eardrops (due to risk of ototoxicity);
keep ear dry (be especially careful with soapy water as it is more likely to enter the canal due to a reduced water tension);
oral antibiotics might be used (amoxicillin is a good choice);
consider an ENT review when the defect is large.
Thank you for reading, keep supporting given below links.
The nose is the most common facial bone to be fractured. The injury involves the nasal septum. This structure is composed of the vomer, the nasal bone and the cartilaginous quadrangular cartilage. A blow to the inferior nose is more likely to injure the cartilagenous septum. A lateral blow is more likely to injure the nasal bones (superior 1/3 of the nose).
Nose bleeding (or epistaxis) is a relatively common occurrence (and may be due to many different causes). The source of bleeding is rarely visible. This can be difficult to manage on the field of play. Direct compression, the application of Vaseline or packing the nose can all be good strategies. Topical decongestants (like Otrivine) can also be used to help reduce bleeding. Off-the-pitch cautery, using a silver nitrate stick, might be needed.
Examination: Ask the player and their friends whether they feel that their physical appearance has changed. Inspect the external nose and internal structure using a nasal speculum. Careful palpation of the bony structures about the face, an assessment of facial sensation and checking visual fields and eye movements are all important. Always remember to assess for associated injuries.
When inspecting the nose, it is especially important to look for a septal haematoma. Failure to identify these can lead to long-term deformity and morbidity. Haematomas can be confused with the inferior turbinate, especially when they are bilateral. When probed, a haematoma is soft as compared with the firm texture of the neighbouring nasal septum. Haematomas need drainage and packing by an ENT surgeon.
Investigations: In cases where a “simple” nasal fracture is suspected, no imaging is needed. Facial X-rays are generally not helpful as they have poor sensitivity and specificity and are frequently confusing. Facial CT is much more reliable when a more significant bony injury (i.e. a facial fracture) is suspected.
Treatment: It is almost always acceptable to treat the player with regular decongestants and review in two days. In the acute setting, where significant deformity exists, consider closed manipulation using a gloved hand. There is, however, no good evidence favouring early reduction of simple nasal fractures.
In most situations, it is usually preferable to allow several days for any swelling to improve. Reduction should be done within 5-10 days. This can be done by both open and closed methods.
Return to play following nasal fracture: Best practice in this area is somewhat debatable. In most cases, fracture healing occurs within three weeks. Ideally, the player should avoid contact during this time. Some athletes will, however, decide to accept the deformity and continue playing. Thermoplastic facemasks can be used to help protect the injury.
Any septal deviation can be treated as a delayed procedure. This may be required for cosmetic and functional reasons.
Thank you for reading , keep supporting given below links.
Injuries to the eye have not been considered elsewhere in this diploma course. Despite this, injuries to the eye are relatively common – and are largely preventable. It is important to have an awareness of common injuries and to have an approach to managing them. It is very important to be able to recognise indications for further evaluation.
Read more about how to approach an eye injury, or problem, in a football player.
History: The mechanism of injury can help to determine the probability of serious problems being present. High-velocity trauma (such as a punch or elbow to the eye) has the potential to cause a penetrating eye injury or orbit fracture (and should be taken very seriously). Dust from other foreign material falling, blowing or being rubbed into the eye will most likely result in a corneal abrasion. This is a common complaint in beach soccer (where sand frequently causes eye irritation). If there has been no associated trauma, consider possible infectious causes.
Examination: It is essential that the player’s visual acuity is adequately assessed (and documented). Normal acuity does not however exclude injury. The eye should be closely inspected, looking for changes in pupil shape, evidence of bleeding (including conjunctival haemorrhage or hyphaemia). Reactivity to light should also be observed. Eye movements should be checked and visual fields should also be assessed. There may be reduced upwards gaze (due to an entrapped inferior rectus following an orbital floor blowout fracture). Palpate for tenderness and assess facial sensation (a blowout fracture can also cause infra-orbital paraesthesia). The fundus should also be assessed with an ophthalmoscope, although this can be challenging in many football environments.
Treatment: Any player who is found to have reduced acuity, restricted eye movements, severe pain or persisting blurring should be referred for an assessment. Similarly, any player who has a hyphaemia, suspected penetrating injury, globe rupture or who is thought to have a retinal haemorrhage or detachment should be immediately referred for an assessment. More minor injuries, like a corneal abrasion, might be treated with lubricating eye drops, in some cases antibiotic eye drops or ointment or with padding of the eye.
Eye conditions are typically related to trauma, infection or allergic conditions. Dry eyes, especially following international travel, are a common complaint.
You should have equipment to assess and treat eye complaints in your medical bag (or stadium medical room). Suggested medications and equipment include:
Ophthalmoscope
Local anaesthetic eye drops (e.g. Minims amethocaine drops)
Eye patches
Cotton buds for everting the eyelid
Chloramphenicol ointments and antibiotic eye-drops (e.g. tobramycin, gentamycin)
Clinicians should be aware of the some of the more common eye injuries and have an approach to managing them. Learning the specific details of these injuries is beyond the scope of this course.
Click on the following tabs to read some further information about each of these conditions.
Corneal abrasion, Lacerations Sub-conjunctival haemorrhage, Hyphaemia, Retinal haemorrhage and detachment Penetrating eye injury Orbital injuries.
Thank you for reading, keep supporting given below links.
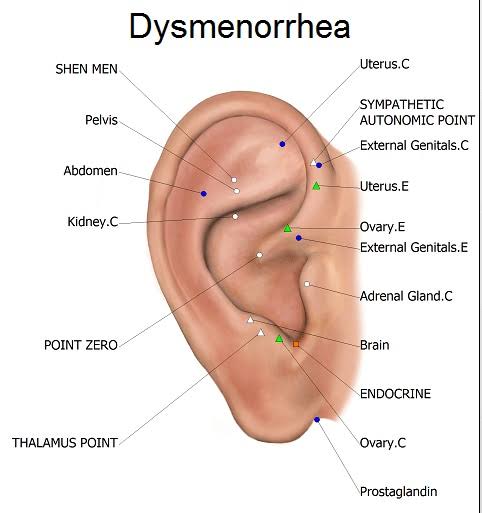
Some women have significant pain and morbidity associated with their menstrual cycle. This can have a significant effect on their ability to play and train. It is a very common complaint among female football players and is often not well managed.
Dysmenorrhea can be classified as either primary or secondary based on the absence or presence of an underlying cause. Secondary dysmenorrhea is dysmenorrhea that is associated with an existing condition. In younger players, painful periods often occur without an underlying problem. In older women, however, it is more often due to an underlying issue (such as uterine fibroids, adenomyosis or endometriosis).
Further assessment or investigations are more likely to be needed in this group. The most common cause of secondary dysmenorrhea is endometriosis.
In most cases, the diagnosis of a dysmenorrhoea is based on a woman’s history and examination. In some cases, a pelvic ultrasound can also be helpful.
Learn more about the treatment of dysmenorrhea in football players.
Symptom: controlWhen faced with a player who has dysmenorrhoea, simple strategies can be used to try to manage their symptoms. NSAIDs are widely prescribed and can be used before training or matches. Heat (a hot water bottle for example) is another useful strategy – but is obviously not practical during training or matches.
Prevention: The oral contraceptive pill (OCP) can be used as a mean of trying to prevent menorrhagia. These treatments work by thinning the lining of the uterus, where prostaglandins are formed, which then reduces uterine contractions and bleeding. The OCP also gives the player the ability to control their menstruation and can also potentially improve the symptoms associated with their period. They may elect to skip the inactive pills if there is an important match or even which coincides with their period.
It is very important that the player’s suitability for the OCP be considered, that all possible side-effects are outlined prior to the medication being started, and that the contraceptive effects be clearly explained.
No negative effect on performance has been found from OCP use. 7 It is, however, important to realise that individuals respond to the OCP differently. As a result, the OCP use should not be started close to a major event.
Some players do not like taking the OCP, or do not have a satisfactory response from this treatment. Another option which might be considered is a Mirena intra-uterine device (IUD).
Thank you for reading, keep supporting given below links.
While blisters appear to be a very minor complaint (relative to other injuries), they can be a major source of morbidity and can prevent a player from being able to train or play. The heel and ball of the foot (the plantar surface of the 1st MTPJ) are generally the most common (and debilitating) locations in football. There are a variety of different strategies that can be used to both prevent and treat this problem.
Closed blister: The following strategy can be used to treat a closed blister. It is important to realise that there are many different ways to do this. Clinicians are encouraged to develop their own strategies. When faced with a painful blister which is likely to limit a player’s ability to compete, follow the following steps:
drain the fluid with a needle and syringe;
inject into drained blister space with diluted betadine (not full strength) and leave in until it stops stinging;
drain out betadine solution;
the blister should be flat and sticking (down due to tackiness of betadine);
dry skin for 30-60 seconds;
create a foam donut and place around the blister;
cover the hole in the foam donut with 2nd skin (or similar);
secure the whole dressing with hypafix tape (or similar).
Open blister: An open blister should be carefully cleaned with antiseptic soap and then dried. Ideally it should be left open when not training (at night, for example). During training, the injured area can also be offloaded by making a foam donut (as described above).
Some practical strategies to try to prevent blisters from occurring include:
carefully break in new boots (and other footwear) by alternating between new and old boots;
do not take new boots to tournaments;
choose the right socks;
wear different pairs of boots and shoes;
keep your feet dry;
tape problem areas (before blisters occur);
be especially careful during pre-season.
Thank you for reading, keep supporting given below link.
Bleeding wounds, from abrasions and lacerations, can occur during football matches. Skin wounds are the fourth most common injury in youth football. Scalp and facial lacerations can be particularly challenging as they frequently cause excessive bleeding.
The Laws of the Game: regulations for bleeding wounds
Any player bleeding from a wound must leave the field of play. They may not return until the referee is satisfied that the bleeding has stopped. A player is not permitted to wear any clothing with blood on it.
The vast majority of wounds seen on a football pitch are minor. Abrasions and small laceration are by far the most common of these injuries. Wounds
with capillary or venous bleeding are typically minor. Capillary bleeding is usually painful and the bleeding is slow but may be persistent. The amount of bleeding is directly proportional to the area of the skin involved. In football, these wounds are most commonly seen when playing on artificial turf.
Wounds with venous bleeding occur as a result of either lacerations or deep puncture wounds. The bleeding flow may be minor to major, depending on the size of the traumatised veins.
Wounds with arterial bleeding are a critical medical emergency and must be promptly recognised and managed. Bleeding is brisk, rapid and pulsatile. Once recognised, the bleeding must be immediately controlled by using whatever means are available. Direct pressure, elevation of the affected limb or wound closure can all be effective strategies. In some cases, an appropriate arterial tourniquet might be used.
Thank you for reading, keep supporting given below link.
While most players who complain of muscle cramps and muscle pain have a benign cause, these symptoms can be related to more significant medical conditions. These might include metabolic diseases or autoimmune conditions or be related to neurological conditions.
It is important to have an approach to assessing players who present with recurrent, or more significant, muscle pain. The following steps might help with this process.
History: It is important to make an assessment of the location of pain and any precipitating factors. It is also important to quantify the player’s overall loading (i.e. whether there have been any changes). Asking about any associated symptoms including weakness and myoglobinuria (coke-coloured urine) is important. When the pain occurs is also an important factor. Pain that occurs shortly after starting training may indicate McCardle disease, while pain that develops after about 30 minutes of training is more suggestive of carnatine palmitoyltransferase deficiency. Whether the symptoms also occur at rest is an important factor.
Enquiring about the player’s past medical history, family history and medication use is also important.
Examination: An examination of the neurological and musculoskeletal systems is needed. Palpate for tenderness and assess muscle strength. Proximal muscle weakness often reflects a metabolic myopathy.
Investigations: Baseline investigations should include the following laboratory tests:
FBC
Electrolytes
CK
TSH
ESR/CRP
Fasting glucose
In some situations, imaging studies can be helpful. Myositis can be demonstrated well on MRI. Neuropathic causes can also often be identified on MRI.
Treatment: In most cases, players with more significant muscle pain, or with more refractory symptoms, should be referred for further assessment. Referral to a neurologist is generally the best next step. This is particularly important when there is abnormal neurology or elevated CK at rest. Further evaluation may include EMG studies, a forearm ischaemic test or high-tech imaging.
Metabolic disease
Two of the more common metabolic causes of muscle pain are McArdle disease and carnatine palmitoyltransferase deficiency (CPT deficiency). These can be distinguished based on their history, examination and investigation findings. Review the following table to learn more about the presentation of these conditions.
Thank you for reading, keep supporting given below link.
Delayed onset muscle soreness (DOMS) is a term used to describe the muscle pain felt after a training session. While this is a normal phenomenon, it can be quite significant and can limit a player’s ability to play or train. The pain typically starts 12 hours after exercise, peaks at 24-48 hours and is finished after about five days. It is generally associated with eccentric exercise or with unaccustomed exercise. Running downhill is a common cause.
Examination: Clinical signs might include finding painful and tender muscles, swelling and increased muscle girth, reduced passive stretch and reduced muscle strength. Exercise performance while suffering from DOMS may also be reduced.
Investigations: No investigations are typically required. Following exercise, especially eccentric exercise, there is an increase in creatine kinase (CK). This is normal. The magnitude of this increase is very variable and so the absolute total is not useful for predicting severity. The peak CK value occurs two days after activity and is gone after 5-7 days.
Treatment: Symptomatic treatment can help for acute episodes. Passive stretching, massage and other soft-tissue techniques can all provide symptom relief. Cold water immersion (ice baths) are also widely used – despite there being little evidence to support the efficacy of this practice. 4 Simple analgesia can also be used in some cases. Explaining that these symptoms are benign and outlining ways in which future episodes can be prevented is also important.
As with cramping, DOMS can also be prevented. The best strategy is training. If a player starts regularly participating in the type of exercise that has caused their symptoms, the probability of developing DOMS is dramatically reduced. Ensuring that the player warms up appropriately prior to training is also important.
Thank you for reading. Keep supporting me given below link.
“Growing up, I used to love playing gully cricket with my brother and his friends– I’d always hit the ball with my foot and everyone would tease me. They’d also play football– I watched their match once and was hooked. There, the coach asked me, ‘You want to play?’ I enjoyed it so much that I ended up playing for 3 hours.
Nadiya Nighat
It was late by the time I got home; Ammi was looking for me. When she saw me returning with the boys, she yelled– ‘Why did you go alone with so many boys?’ When I told her I was playing football, she was furious– ‘Yeh ladko wale khel nahi khelne chahiye!’ Bahut maar padi thi uss din. But I spoke to Abbu and told him how good I was at the game, even better than the boys– he agreed and persuaded Ammi. I enrolled myself in a football training camp.
I was 1 girl amongst 47 boys– my neighbours would tease, ‘Ek ladki ladko ko nacha rahi hai.’ They’d taunt my parents, ‘Why are you allowing her to dress like this?’ They even forbade their daughters to be friends with me. I didn’t care– I was playing football!
But the boys I was training with said, ‘Why don’t you stay home and wash utensils like other girls?’ My coach gave them an earful, ‘I can lose you all but won’t let Nadiya go.’ That day, I learnt that I had to toughen up to survive in a man’s world. In 2010, I played my first national tournament at 14; my team won because of me. Around the same time, I got a boy cut and stopped wearing a hijab while playing– I wanted to fit in and dodge my neighbours’ scornful eyes. But the discrimination didn’t stop.
At a local tournament, I was the only girl and had to hide my identity. A man in the audience figured it out and demanded that I stopped playing. Even though I was crucial in winning the semi-finals. I wasn’t allowed to play the finals… because I was a girl.
My family also believed that there was no scope for a woman in football. I was shattered– but my coach pushed me to start a training centre of my own while I made a place for myself as a player. So, I approached the J&K football association– they let me use their ground and equipment. At first, only boys enrolled. So, I’d go to schools to motivate girls to play. While I pushed the association for an all women’s team, my career picked up– in 2018, I became the first Kashmiri female captain of the J&K football team. Ammi and Abbu were so proud. But all my efforts bore fruit when Real Kashmir FC launched an all women’s team!
Still, recently, somebody commented on my post– ‘This game is not for cultured women,’ but I don’t care anymore. I train over 40 girls in my centre. Looking at me, many of them got a boy cut to ‘fit in’, so I decided to put an end to it. I let my hair grow long because that’s how I want it– why can’t I be me AND do what I love?”
Source~ (via Humans of Bombay)
Thank you for reading, keep supporting given below links.
Exercise-associated muscle cramps (EAMC) are among the most common problems encountered by a clinician looking after football players. This problem typically happens only during extreme exertion and is far more common during games than during training sessions. Some players frequently experience cramps while others do not. As a result, it seems likely that there is a genetic component to cramp (a predisposing gene has also been identified).
The fact that many players describe a family history of cramp also supports this hypothesis. Older players also seem to be at an increased risk of cramping. There is very little evidence to support the widely held belief that cramp is caused by either dehydration or electrolyte abnormalities. It appears to be a direct consequence of muscle fatigue.
Cramp typically involves muscles which cross two joints (like the calf, hamstrings or quadriceps). There is often a prodromal – “cramp prone state” – when the muscle feels vulnerable which precedes the onset of symptoms. During this time, the player may have a sense of tightness or muscle pain or be apprehensive that cramp is imminent.
Investigations
No specific investigations are generally required. This is a clinical (rather than radiological or laboratory) diagnosis.
Treatment
The acute, on-field management of muscle cramps involves stretching the involved muscle with contraction of the antagonist. Once the player has developed cramp, however, it is very likely that they will be substituted.
Given that acute muscle cramping can be difficult to manage, it is important to try to prevent this from happening. The key strategy involves being adequately prepared and conditioned.
Thank you for reading , Keep supporting given below links.
There are a variety of relatively minor complaints that commonly occur on the touchline – or present in the dressing room – which are not considered in the other modules in this course. These conditions include the management of blisters, muscle cramps and minor bleeding. While quite minor, each of these problems can cause significant morbidity and prevent a player from reaching their potential or participating in the game they love.
Conditions involving the eye, ear and nose are also considered in this module. These injuries can be more significant and need specialist care. The definitive management of many of these conditions is beyond the scope of this course. It is, however, important to have an awareness of some of the potential complications associated with each and to be able to refer affected players for a further assessment.
Mr. Jatin Tyagi (Coach is lifelong student)
In this module, we will consider how a range of more “minor” medical issues can be managed and consider how a clinician might be able to allow a player to continue to safely participate in football training and matches.







; Some Foods You Can Eat")