Lesson 5:-
Chest injuries in football are almost exclusively limited to chest wall muscle tears and fractured ribs, when such rare events do occur. The mechanism of injury for fractured ribs is contact against a hard object. Common injury mechanisms include a direct blow from an opponents elbow, a hard landing onto the field of play or collision against the goalposts. Whatever the mechanism of chest wall injury, most injuries cause severe pain, and removal from the field of play is usually warranted, either temporarily or for the duration of the match, unless the chest wall can be adequately strapped to alleviate the pain and allow functionality once again.
Chest trauma
Chest trauma most commonly occurs after a direct blow – most often with an opponent.
Two type :- Rib Feature & tension pneumothorax
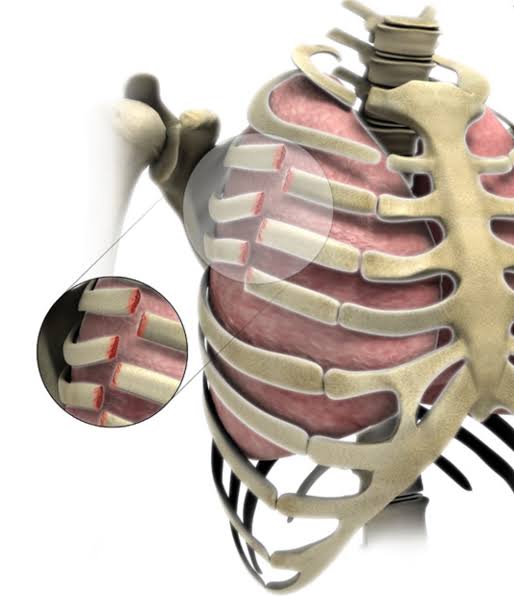
1. Rib fractures
Rib fractures are the most common injury sustained following blunt chest trauma. They account for more than 50% of all thoracic injuries from non-penetrating trauma. Approximately 10% of all patients admitted after blunt chest trauma have one or more rib fractures. These fractures are rarely life threatening but can be a sign of a more severe visceral injury inside the abdomen and the chest. Fractures generally occur at the site of impact or the postero-lateral bend, where the rib is weakest.
History:-
Patients who have fractured a rib/ribs typically present with significant pain related to the affected area. They often have pain with breathing (particularly inspiration).
Examination:-
The typical signs of a rib fracture include visible distress, pain on manual compression of the rib(s) over the affected site and the presence of bruising or swelling over the fracture site. It is very important to consider the possibility of a more significant injury. Assess the player post injury for alertness, adequacy of the airway, breathing and circulation status. You should also assess the lung breath sounds bilaterally to ascertain if a clinical pneumothorax is present.
A fractured rib may tear the visceral pleura and underlying lung and cause a pneumothorax. This may not be clinically detected if small – or it may be larger and present clinically with decreased breath sounds found on auscultation and increased resonance on percussion on the affected side. Should this occur, a decision must be made regarding management of the pneumothorax, if at all.
Investigation:-
In some situations, rib fractures are not well demonstrated on x-ray images. When an x-ray appears normal, but there are clinical signs suggestive of a fracture, the player should generally be treated symptomatically – rather than pursuing further imaging. A chest x-ray series can generally demonstrate a pneumothorax well. CT imaging is generally the next best study. Monitoring pulse oximetry or checking arterial blood gases may be required when there is a pneumothorax.
Treatment:-
Uncomplicated rib fractures can generally be managed symptomatically. The player may be allowed to continue as long as they are comfortable. Analgesics and chest wall strapping may provide some assistance. These injuries are generally very painful and usually prevent players from returning to competitive football for four to six weeks. If there are signs of a pneumothorax, or other associated internal organ injury, then the player should be urgently transferred to the nearest, most appropriate medical facility, with the addition of supplemental oxygen via face mask during ambulance transfer.
Pneumothoraces can be treated with observation (when small), aspiration and small-bore catheter insertion. These treatments are effective, take less time and have fewer complications when compared with inserting a chest drain.
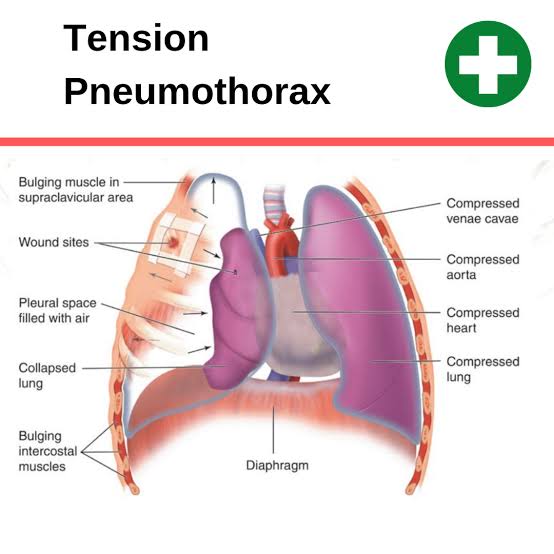
2. Tension pneumothorax
If the fractured rib(s) have resulted in a clinical pneumothorax with deteriorating symptoms and signs, the presence of a tension pneumothorax must be considered, clinically sought and, if present or in any doubt, requires urgent treatment. This rare but life-threatening medical emergency is caused by a tear in the lung airways, such that during inspiration, air escapes into the pleural space, while during expiration the air is trapped inside the pleural space, due to a valve-like mechanism. This results in successive volumes of air entering the pleural space slowly compressing the unilateral affected lung, then compressing the mediastinum until the heart itself is pushed to the opposite side from the increasing pleural pressure. Once the heart is moved, compression and closure of the superior and inferior vena cavae may occur, decreasing venous return to the right side of the heart and thereby decreasing cardiac output, leading to severe hypovolaemic shock and eventually non-output cardiac arrest.
History:-
Any player who appears short of breath or tachycardic at rest (following chest trauma) should be assumed to have a tension pneumothorax. Signs of shock should also be taken very seriously.
Examination:-
In addition to signs suggesting shock following a chest injury, the following findings should prompt a diagnosis of a tension pneumothorax.
- Decreased or absent breath sounds on the affected side
- Hyper-resonance to digital percussion on the affected side
- Distended neck veins
- Displacement of the cardiac apex beat to the non-affected side
- Deviation of the trachea to the non-affected side
InvestigationsIf there is clinical evidence or even a suspicion of a tension pneumothorax being present from the clinical picture of the patient, immediate treatment must be undertaken to decrease the pressure within the affected pleural space.
One must never refer the patient for radiological investigation in order to confirm the diagnosis, because this may lead to cardiac arrest from delayed release of life-threatening intra-pleural pressure. Tension pneumothorax is always a clinical diagnosis and should never be seen on a radiological investigation.
Emergency treatment:-
Treatment of a tension pneumothorax is aimed at immediately decreasing the raised intra-pleural pressure, thus allowing the displaced heart to return to its original position with opening of the superior and inferior vena cavae, and thus restoration of venous return and hence cardiac output. This is achieved by making a hole in the chest wall into the pleural cavity and thus releasing the entrapped gas under pressure. This can be undertaken by inserting a standard 5-cm long, large bore (16G / 14G) intravenous catheter needle. This should be done into the affected pleural cavity in the fourth or fifth intercostal space, immediately above the rib perpendicular to the skin, in the vicinity of the anterior or mid axillary line. This location is selected because the thickness of the chest wall at the anterior mid axillary line is 1 cm thinner than that at the traditional second intercostal space, mid-clavicular line.
Follow these steps to successfully manage a tension pneumothorax.
- Place the player in either a lateral recumbent position with the affected side up, or supine, with the head of the bed up 40-45 degrees.
- Identify the fourth or fifth intercostal space in the anterior axillary line.
- Prep the area.
- Insert the 14- or 16-gauge catheter needle just above the rib, perpendicular to the skin. As you traverse the pleura, you may hear the distinctive rush of air from the decompressed tension pneumothorax.
- Remove the needle and leave the catheter in place, securing it to prevent dislodgment.
- Re-evaluate the patient to ensure a positive clinical effect and continue to monitor the patient closely as you complete the evaluation and resuscitation.
- Treat the residual “simple pneumothorax”
Although air may escape under pressure from the catheter, these are known to kink or displace fairly easily, and therefore the patient must be constantly monitored until safe arrival in an emergency department where radiological investigations can be undertaken to determine the exact diagnosis, and be treated accordingly.
Thank you for reading, keep supporting given below links.

