Lessons 4:-
Abdominal injuries in football are an uncommon event; however, they appear to be happening more frequently. Abdominal injuries do not present as obviously as many orthopaedic injuries, because of the internal and concealed locations of the intra-abdominal organs. A high index of suspicion and knowledge of the mechanism of injury may contribute to the earlier diagnosis of acute, serious abdominal injuries.
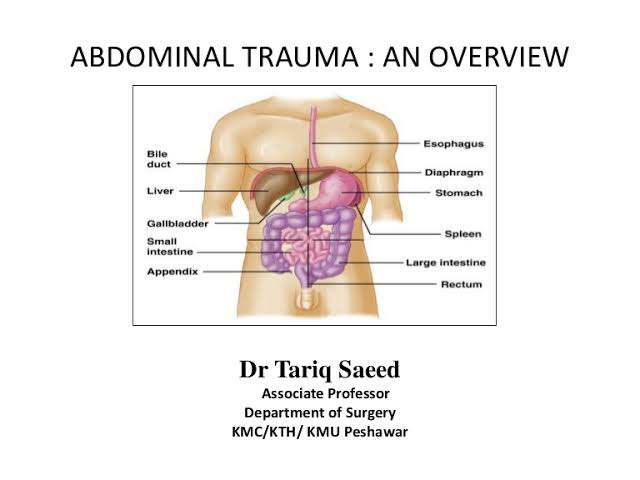
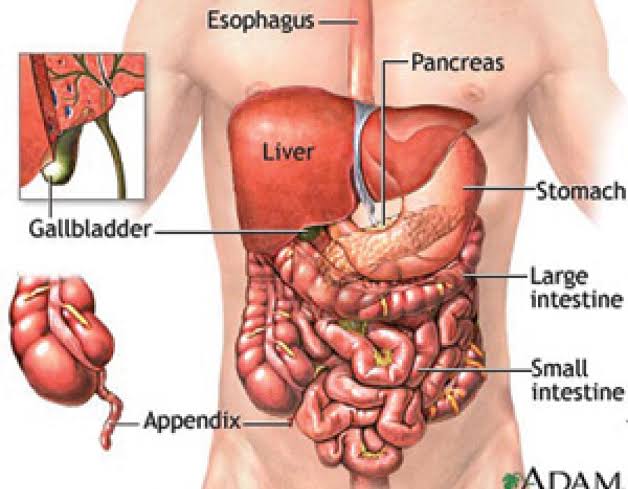
Blunt trauma to the abdomen may cause injury to the solid organs of the abdomen, namely the liver, spleen or possibly a kidney, resulting in intra-abdominal haemorrhaging.
This can potentially be life threatening, depending on the extent of the haemorrhage. The injured player may present with relatively modest pain initially and over time develop hypovolaemic shock as the haemorrhage increases. The hollow organs (e.g. the jejunum colon and duodenum) can also be injured.
History:-
Pain may occur after an abdominal injury, but this does not always occur. Pain may not occur until signs of peritonitis develop hours after the injury.
Examination:-
The traditional examination of the abdomen, including inspection, palpation, percussion and auscultation, may reveal bruising, tenderness, guarding and loss of bowel sounds. The player should be assessed for evidence of shock, although signs can develop over time. This is especially common following the rupture of a hollow organ. Serial physical examinations have been shown to be a sensitive way to detect early intra-abdominal haemorrhage and are a practical way to assess these players.
Investigations:-
In general terms, any player who is suspected of having an injury to an intra-abdominal organ should have a CT scan. Ultrasound scans, including FAST scans, can be a helpful initial study. X-rays are not generally useful but may show pneumoperitoneum or obliteration of the psoas shadow (when there is a retroperitoneal haematoma). Baseline blood tests, including a cross match, should be taken. It is important to especially consider the patient’s haemoglobin.
A mid-stream urine test is also useful when an injury to the genitourinary tract is suspected.
Treatment:-
Injured players in hypovolaemic shock are managed like any other patient in shock with protection of the airway, supplemental oxygen administration, if present, intravenous access and limited crystalloid administration sufficient to maintain a blood pressure at 90mmHg and an appropriate diluted, titrated infusion of an intravenous analgesia with emergent transfer to hospital. Hypotensive resuscitation is preferred in such patients, because injudicious use of large quantities of intravenous crystalloids may result in increasing the blood pressure at the bleeding site and worsen the bleeding. Therefore, the sooner the player is transferred to hospital and under the care of a surgeon the better.
Once a diagnosis has been made, a decision must be made about whether the injury requires surgical management. In many cases, liver and spleen injuries can be managed non-surgically.
Thank you for reading. Keep supporting given below links.

