Lesson 3:-
Severe anaphylaxis is an acute life-threatening allergic reaction. The risk of anaphylaxis in the football environment, both on and off the field of play, needs to be appreciated. Known trigger factors include food, medications, hymenoptera stings, fever and infections (such as upper respiratory tract infection). The risk of anaphylaxis may also be increased by “cofactors” that include non-steroidal anti-inflammatory medications (NSAIDS), exercise and alcohol. All of these precipitants may be relevant to the football environment. Travel into unfamiliar environments, particularly with regard to the consumption of food and drink, may increase the risk of severe allergic reactions.
The ability to recognise and manage anaphylaxis must be within the scope of team doctors and football stadium medical services.
History and examination
Prompt recognition and immediate treatment is essential in anaphylaxis. The following clinical criteria, adapted from the World Allergy Organisation Guidelines, are relevant within the football environment.1-3
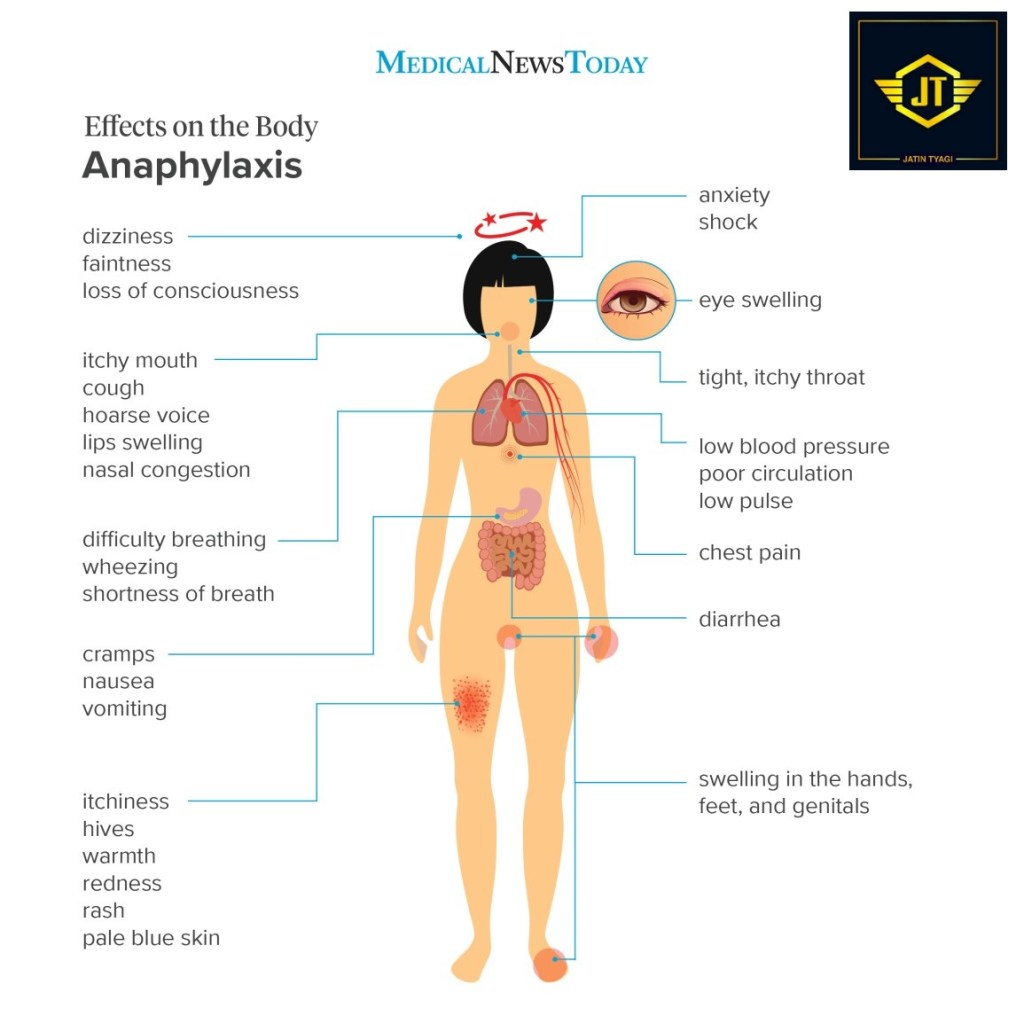
Anaphylaxis must be considered when any one of the following clinical criteria is present:
Acute onset of illness involving the skin, mucosal tissue or both (e.g. general urticaria, itching, redness, swollen lips, tongue or uvula)
AND
At leastoneof the following clinical syndromes:
- Respiratory – dyspnoea, wheezing, stridor, hypoxaemia
- Cardiovascular – reduced blood pressure, syncope, collapse
OR
Twoor more of the following syndromes that occur rapidly after known or possible exposure to a likely allergen:
- Acute onset of illness involving the skin, mucosal tissue or both (e.g. general urticaria, itching, redness, swollen lips, tongue or uvula)
- Respiratory – dyspnoea, wheezing, stridor, hypoxaemia
- Cardiovascular – reduced blood pressure, syncope, collapse
- Gastrointestinal – severe cramps, abdominal pain, vomiting
OR
Reduced blood pressure after known or possible exposure to a likely allergen:
- Children – low systolic blood pressure or greater than 30% decrease from normal for age.
- Adults – systolic blood pressure less than 90mmHg or greater than 30% decrease from normal for the person.
Treatment
The key to the successful treatment of severe anaphylaxis in the football environment is early identification, an appreciation of its life-threatening consequences and initiating immediate treatment with adrenaline/epinephrine.
In any situation where any of the above clinical signs or symptoms occur in the context of a possible allergic reaction to food, medications, hymenoptera stings (e.g. bees) or other chemicals, always consider the possibility of anaphylaxis immediately. It is always better to treat the player early rather than await clinical deterioration, as hesitation in the treatment of severe anaphylaxis can be fatal.
The mainstay of treatment of severe anaphylaxis is the administration of epinephrine (adrenaline) by intramuscular administration into the antero-lateral thigh (vastus lateralis).
Epinephrine (adrenaline):-
If an auto-injector (e.g. an EpiPen™) is available, it is used by thrusting the device appropriately against the antero-lateral thigh. This can be done through clothing if necessary. The pen should be held against the thigh for at least 10 seconds to allow full intramuscular injection of the intended epinephrine dose (0.3mg in an adult injector or 0.15mg in a child injector).
If epinephrine is only available in ampoule form as a 1:1000 (1mg/ml) concentration (or repeated doses of epinephrine are required without an additional auto-injector being available), administer 0.5mg (equal to 0.5ml of the 1:1000 epinephrine) intramuscularly (IM) into the antero-lateral thigh in an adult or 0.3mg in a child. Before injecting the epinephrine into the thigh muscle, withdraw the syringe plunger to ensure that the needle is not in a vein, as intravenous concentrated Epinephrine injection can have serious cardiac effects.
If severe symptoms continue after epinephrine IM injection, repeat the dose every five minutes. An ambulance should be called (if not already on site).
If, after epinephrine administration, the patient remains hypotensive (i.e. there is no radial pulse), position the patient supine and elevate the legs. Establish intravenous access as soon as practically possible and consider administering normal saline, or equivalent solution, in order to obtain a systolic blood pressure of 90mmHg minimum. Colloids may be considered, although there is no evidence to substantiate their use. Note that up to 50% of the intravascular volume can be lost within ten minutes in severe anaphylaxis, thus initially requiring potentially large volume replacement.
Beta-2 agonists:-
In the presence of anaphylactic-induced bronchospasm, in addition to epinephrine administration, consider the use of β2-agonist inhalation, either by an inhaler and spacer or via oxygen-powered nebulisation. This treatment can be repeated as often as necessary.
Antihistamines:-
There is no evidence that the administration of antihistamines in severe anaphylaxis has any beneficial effect in the initial management. As a result, it is not suggested as part of the immediate response. Once the patient has been transferred to the nearest, most appropriate emergency department, the use of an antihistamine can be considered after a full medical history and examination has been undertaken, possibly for the relief of urticaria and itching symptoms.
Glucocorticoids:-
There is no evidence that the administration of glucocorticoid medications in severe anaphylaxis has any beneficial effect in the initial management. As a result, it is not suggested as part of the immediate response. Its administration, once the patient has been transferred to the nearest, most appropriate emergency department, can be considered after a full medical history and examination has been undertaken.
The patient should be transferred to the nearest, most appropriate medical facility as soon as possible after the initial dose of epinephrine/adrenaline has been administered, so that further support may be administered by the emergency department, if and when necessary.
Follow-up
Discharge follow-up and educational strategies to prevent further occurrences and treat possible future events may be required from sports healthcare professionals overseeing the healthcare of the team member, where relevant.
Thank you for reading, stay tuned. Keep supporting given below links.

